Download
1 / 38
460 likes | 818 Views
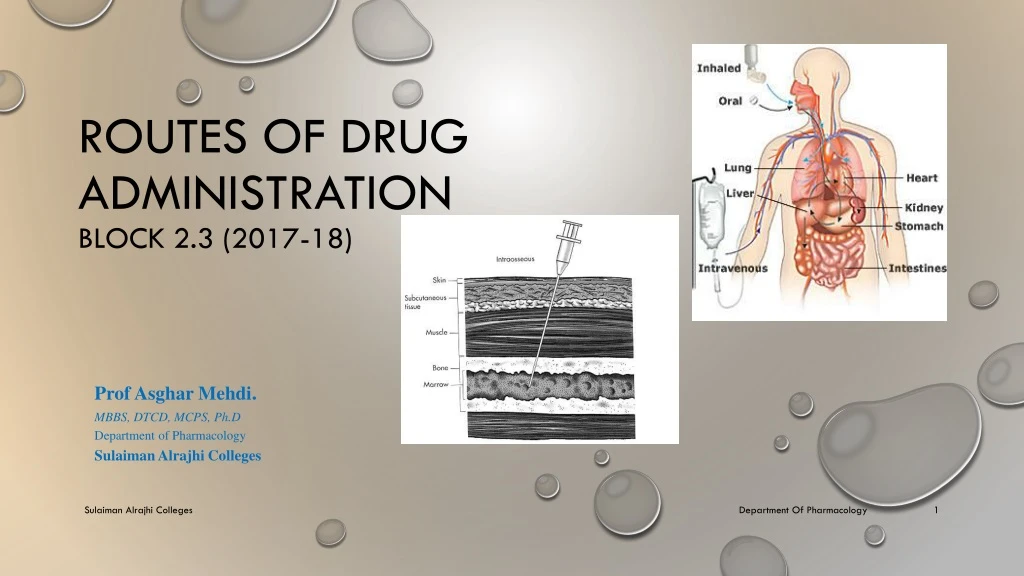
Routes of drug administration Block 2.3 (2017-18). Prof Asghar Mehdi . MBBS, DTCD, MCPS, P h.D Department of Pharmacology Sulaiman Alrajhi Colleges.

E N D
Routes of drug administration Block 2.3 (2017-18) Prof Asghar Mehdi.MBBS, DTCD, MCPS, Ph.DDepartment of PharmacologySulaiman Alrajhi Colleges Sulaiman Alrajhi Colleges
A patient walks into your clinic complaining of chest pain, nitroglycerine the desired medicine is available to you in form of oral tablet, ointment, transdermal patch, spray and sublingual tablet which form would you chose??????????? Sulaiman Alrajhi Colleges
Important Routes of Drug Administration The Route of Administration (RoA) that is chosen may have a profound effect upon the speed and efficiency with which the drug acts Sulaiman Alrajhi Colleges
Objectives • Lists route of administration of drugs • Lists advantages & limitations of each route. • Be able to demonstrate the most effective tool for particular condition. • Be able to administer Intramuscular, Intra Venous & Subcutaneous Injection Sulaiman Alrajhi Colleges
Routes of administration of Drug Sulaiman Alrajhi Colleges
Enteral route • Oral • Rectal • Sublingual • Via feeding tubes • Drugs are swallowed. • Formulation of drugs taken orally include Solid: capsules, tablets, lozenges Liquid: syrups, suspensions, emulsions, mixture Sulaiman Alrajhi Colleges
Advantages of oral route • Most convenient & commonly used, economical. • Does not require sterile techniques for administration. • Rapid and high blood concentration of drug avoided. • Easy recovery of drug if toxic. • Does not require a trained personal for administration • Drugs causing irritation parenterally can be administered • Safest route • Large doses can be given • Largest surface area for absorption Sulaiman Alrajhi Colleges
Disadvantages of the oral route • Rate of absorption is variable / affected by simultaneous administration of drugs like antimuscarinic which inhibit GI motility. • Irritation of the GI mucosal surface can occur • Drug can be destroyed by enzymes, variable pH, intestinal flora • GIT pathologies interfere with absorption • First pass effect occurs • Can not be used in comatose patients • Absorption may be delayed / reduced / enhanced after food intake. Sulaiman Alrajhi Colleges
ENTERIC COATING • The presence of food in the stomach delays gastric emptying, so drugs that are destroyed by acid become unavailable for absorption. • Enteric coating of a drug protects it from the acidic environment; the coating may prevent gastric irritation.
FIRST-PASS METABOLISM • Most drugs absorbed from the GI tract enter the portal circulation and pass through liver before they are distributed into the general circulation. More than 90% of nitro-glycerine is cleared during a single passage through the liver.
Drugs administered orally Some drugs are not absorbed like gentamycin, vancomycin & neomycin and some are destroyed like Insulin and need to be given by other routes. Caution • Verify that the patient is able to swallow and is not nauseating or vomiting • Tablets and capsules • Loprin (asprin) • Panadol (paracetamol) • Amoxil • Syrups and suspensions • Mucaine • Brufen • Calpol • lozenges • Stepsils Drugs which are not absorbed are indicated for GIT infections & sterilization in cases of excessive toxins Neomycin in hepatic failure. Antiheliminthics for parasitic infections, Vancomycin in pseudomembranous colitis Sulaiman Alrajhi Colleges
Sublingual route • Absorption directly from oral cavity. • Rapid response. • If drug unstable at gastric pH or rapidly metabolized by liver. • Escape first pass metabolism. • Formulation of drugs administered:Tablets • Sprays • Angised (nitroglycerine) • Captopril. Nitroglycerine,is extensively metabolized when taken orally (>90%). It is rapidly absorbed through sublingual mucosa, its peak plasma level is reached within 1‐2 minBecauseof short half life (3‐5 min) serum concdeclines rapidly to a level below therapeuticconcwithin 10‐15 min. Sulaiman Alrajhi Colleges
sublingual route Advantages Disadvantages • Fast absorption • First pass effect minimized • GI tract enzymes and ph variability bypassed • Excess drug can be removed • Large doses can not be given • Repeated administration cause mucosa irritation • Vasoconstrictions drugs can not be given • Unpleasant taste of some drugs • Drugs must not be swallowed or chewed • It should dissolve completely before eating or drinking anything Sulaiman Alrajhi Colleges
Drugs administered rectally • Better absorption • Self administration • Privacy must be ensured May be used in cases of emergencies Drugs absorbed from lower rectum and avoids portal system as it drains directly into systemic circulation. First pass effect is unpredictable. Some times used in cases of proctitis or colitis. Sulaiman Alrajhi Colleges
rectal route Advantages Disadvantages • Can be given when oral administration impractical • Bypasses GI enzymes and ph variability • First pass effect minimized • Can be given to uncooperative, comatose and young patients • Can be administrated vomiting patients • Patient feels embarrassed • Many drugs are irritant to the mucosa Sulaiman Alrajhi Colleges
Drug administration via feeding tubes • For patients who can not swallow but have a functional GI tract • Administration is done through naso-gastic tube or gastrostomy • Drug given should be liquid form or crushed tablet in a liquid vehicle Sulaiman Alrajhi Colleges
PARENTERAL ROUTE Advantages Demerits • Active delivery of drug. • 100% bioavailability. • Effective dose more accurately delivered. • Emergency route! Quick action • For drugs that have irritant effect on GIT. • Most control over drug dosage. • Chances of sepsis or phlebitis! Spread of infectious diseases • Painful - extravasation - irritant. • Difficulty in self administering. • In-adverent risk of self administration. • Expensive! • I am like a bullet from a gun…once fired…you cant retreat! Sulaiman Alrajhi Colleges
INTRA-VENOUS & INTRA-ARTERIAL • Mostly deliver aqueous solutions. • Provide effect in just about….10-12 secs! • Control the drug delivery and its accuracy as well. • Smallest and the largest doses we can deliver! • Is not effected by liver metabolism - 100% available! • Can give “GIT irritating” drugs Sulaiman Alrajhi Colleges
Painful! INTRAMUSCULAR • Pain. • Sepsis. • Toxic dosage. • Thrombosis. • Oily solutions are PAINFUL. • No retreat! Sulaiman Alrajhi Colleges
INTRAMUSCULAR Merits Demerits • Painful! • Injury to nerves – risk of paralysis! • Administered dose can not be retaken. • Good in emergency. • When vein is poor or cannot be maintained. • Mostly in infants but adults aren’t left out! • Technically easier than Intra-venous. • Absorption is faster! • Drugs in oil bases can also be given! Sulaiman Alrajhi Colleges
SUBCUTANEOUS Limitations! Merits • Used only for drugs not irritating to the tissues! • The absorption is slow as compared • Repeated injections at same site cause lipodystrophy. • Less painful than her cousin intra-venous. • Uniform and sustained drug delivery. • Self medication is possible. • Depot (oily) preps can be given for prolonged action. • Rate of absorption may be varied. Sulaiman Alrajhi Colleges
DERMOJET • A gun is used to deliver the drug to the superficial layers of skin with a high velocity jet through a micro-fine orifice. • Fine needles means to minimize pain! • Suited for mass inoculations! • E.G.: Insulin for diabetes mellitus patients also Insulin PENS PELLET IMPLANTATION! • Drug in a solid pellet is implanted under the skin. • Requires a trocar and a canula. • Provides sustained release of the drug over weeks and months! Hormone preparations. Sulaiman Alrajhi Colleges
Methods for delaying absorption. • Adrenaline is added to local anesthesia caused vasoconstriction - minimizes bleeding & delay absorption – prolongs action of anesthesia. • Esterification of steroid hormones & antipsychotic drugs increases their solubility in oil & slows their rate of absorption. • Subcutaneous implants . Sulaiman Alrajhi Colleges
INTRA-DERMAL • Used for vaccination. • Mostly used for delivering antigens, vaccines for stimulating immunity in malignancies, bladder carcinomas, allergic disorders. • Don’t mistake it for subcutaneous…they may seem alike but are different! Limitations • Only small doses of drugs can be injected. • Skin should be tight. • Volume of drug should be such that it doesn’t penetrate the soft tissue. • Often accidental delivery into the subcutaneous region! Sulaiman Alrajhi Colleges
INTRA-THECAL • Via the cerebrospinal fluid! • The site is mostly the epidural space! Used in labor & delivery. • Steroids, also methotrexate in acute lymphocytic leukemia! • Used in spinal anesthesia. • Baclofen relieves muscle spasm - post operative analgesia – pca patient controlled analgesia. Sulaiman Alrajhi Colleges
OTHER : INTRA-CARDIAC INTRA-ARTICULAR Sulaiman Alrajhi Colleges
INHALATION: breathed into the lungs, usually through the mouth • Is used for volatile & gaseous anaesthetics with lungs serving as both route of administration & elimination. • Drugs used for their effects on lungs - aerosols – steroids, bronchodilators. • Smaller droplets go deeper, which increases the amount of drug absorbed • Inside the lungs, they are absorbed into the bloodstream • Sympathomimetic & ipratropium (muscarinic receptor antagonist) have low incidence of systemic adverse effects – poor absorption in systemic circulation more of local effects. Sulaiman Alrajhi Colleges
INHALATIONAL Advantages Disadvantages • Early onset of action, 7-10 seconds. • User can titrate (regulate the amount of drug they are receiving) • ROUTE OF CHOICE - EXTENSIVELY USED IN ASTHMA • Most difficult route of administration because requires coordinated efforts • Patient compliance • Improper use can lead to candida infections of oral cavity. Mostly steroids administered in asthma • Particles smaller than 0.5 micron in use, larger than 20 micron would get impacted in mouth and throat. Sulaiman Alrajhi Colleges
Spacer Maximizing airway deposition of a pMDI-delivered drug requires a slow (30 L·min−1), deep inhalation commencing immediately after pMDI activation followed by a breath-hold pause of ≥4 s and optimally up to 10 s.Even with optimal technique and modern hydrofluoroalkane propellants, however, pMDIs deliver, at best, only ∼20% of the emitted dose to the lower airways, leaving ∼80% in the oropharynx. With suboptimal or incorrect technique, this fraction is further reduced, potentially to zero. WalterVincken, Mark L. Levy, Jane Scullion, Omar S. Usmani, P.N. Richard Dekhuijzen, Chris J. Corrigan, Spacer devices for inhaled therapy: why use them, and how?, ERJ Open Research 2018 4: 00065-2018; DOI: 10.1183/23120541.00065-2018 Nebulizer Spacer Sulaiman Alrajhi Colleges
INTRANASAL: sprayed into the nose and absorbed through the nasal membranes • Examples: • Nicotine (for smoking cessation) • Calcitonin (for osteoporosis) • Sumatriptan (for migraine headaches) • Corticosteroids (for allergies) • Sprayed into the nose and absorbed through the nasal membranes • The drug must be transformed into tiny droplets in air (atomized) • Once absorbed, the drug enters the bloodstream Advantages: • Painless & ease of use • Avoids first pass metabolism. • Nose-brain pathway allows direct delivery • to the cerebral spinal fluid Disadvantages: • Limited medications that can be delivered in this fashion • Many medications are not adequately concentrated to achieve ideal dosing volumes • Mucosal health impacts absorption Sulaiman Alrajhi Colleges
TOPICAL: applied to the skin (cutaneously) for a local (topical) effect • Includes application to the skin or mucous membrane of the eyes, nose, throat, airways, or vagina • The rate of absorption varies with the area of application and drugs formulation • It is usually slower then any other routes of administration • Used widely when a local effect is desired or to minimize systemic affects especially in dermatology and ophthalmology • Drugs aren’t absorbed in the blood circulation. It remains in the applied local area and gives its effect there only. Sulaiman Alrajhi Colleges
Advantages • Easy administration • Avoid first-pass effect Disadvantages • Few allergic reactions • Difficult to deliver precise dosage • May stain patient’s clothing & bed linens • Distinctive smell of some drugs • Examples: • Clotrimazole: applied as a cream directly to the skin in the treatment of dermatophytosis • Atrophine: installed directly into the eye to dilate the pupil to permit measurement of refractive errors Sulaiman Alrajhi Colleges
TRANSDERMAL: delivered through the skin by a patch • Transdermal patches, mixed with a chemical such as alcohol that enhances penetration of the skin, pass through the skin to the bloodstream without injection • Through a patch, the drug can be delivered slowly and continuously for many hours or days or even longer. As a result, levels of a drug in the blood can be kept relatively constant • Patches are particularly useful for drugs that are quickly eliminated from the body because such drugs, if taken in other forms, would have to be taken frequently Sulaiman Alrajhi Colleges
Transdermal ADVANTAGES DISADVANTAGES • However, patches may irritate the skin of some people. In addition, patches are limited by how quickly the drug can penetrate the skin. Only drugs to be given in relatively small daily doses can be given through patches • Transdermal delivery is safer, more efficient, more convenient and less painful than injections or IV’s. • Examples of such drugs include nitroglycerin (for chest pain), scopolamine (for motion sickness), nicotine (for smoking cessation), clonidine (for high blood pressure), and fentanyl (for pain relief). Sulaiman Alrajhi Colleges
Route for administration -Time until effect- Important • intravenous 30-60 seconds • intramuscular 10-20 minutes • subcutaneous 15-30 minutes • inhalation2-3 minutes • sublingual 3-5 minutes • rectal5-30 minutes • ingestion 30-90 minutes • transdermal (topical) variable (minutes to hours) No single method of drug administration is ideal for all drugs in all circumstances Sulaiman Alrajhi Colleges
References: • Introductory clinical pharmacology by Sally.S.Roach • Pharmaceutical practice by Arthur .J. Winfield • Drug therapy in nursing by DianeS. Aschenbrenner • Basic & clinical pharmacology Katzung 13 th edition • Lippincott’s pharmacology 6th edition. • Rang & dale 8th edition • Clinical pharmacology 11th edition peter Bennett Sulaiman Alrajhi Colleges