Download
1 / 106
1.07k likes | 1.33k Views
Pathogenesis of diseases of the Pituitary, Pineal,Thyroid and Parathyroid glands. Trinity Medical School Dublin Dr. B. Loftus. Endocrine System. Highly integrated group of organs that maintains metabolic equilibrium Hormones act on distant target cells-concept of feedback inhibition

E N D
Pathogenesis of diseases of the Pituitary, Pineal,Thyroid and Parathyroid glands Trinity Medical School Dublin Dr. B. Loftus
Endocrine System • Highly integrated group of organs that maintains metabolic equilibrium • Hormones act on distant target cells-concept of feedback inhibition • Endocrine disease may be due to underproduction or overproduction of hormones, or mass lesions
Pituitary Gland anterior posterior
Pituitary Gland- microscopic adenohypophysis neurohypophysis
Adenohypophysis acidophils basophils chromophobes
Adenohypophysis:cell types • Acidophils secrete growth hormone (GH) and prolactin (PRL) • Basophils secrete corticotrophin (ACTH), thyroid stimulation hormone (TSH), and the gonadotrophins follicle stimulating hormone (FSH) and luteinizing hormone (LH). • Chromophobes have few cytoplasmic granules but may have secretory activity
Cell population of the anterior pituitary • Somatotroph (GH)50% (acidophils) • Lactotroph (PRL) 20% (acidophils) • Corticotroph (ACTH) 20% (basophils) • Thyrotroph/Gonadotroph 10% (basophils) (TSH/FSH/LH)
Neurohypophysis • Resembles neural tissue with glial cells, nerve fibres, nerve endings and intra-axonal neurosecretory granules • ADH (antidiuretic hormone, vasopressin) and oxytocin made in the hypothalmus are transported into the intra-axonal neurosecretory granules where they are released
Control of Anterior Pituitary Function The Neuroendocrine Axis • Cerebral cortical effects on hypothalamic nuclei • Hypothalamic releasing and release-inhibiting factors • Ambient levels of target-organ hormone product
Causes of Pituitary Hypofunction • Infarction: Post-partum (Sheehans syn.) DIC Sickle cell anaemia Temporal arteritis DM/hypovolaemia Cav. sinus thrombosis • Compression: Non-functional tumour Craniopharyngioma Teratoma • Infection: TB meningitis
Symptoms and Signs of Pituitary Hypofunction • Acute (adult): apoplexy failure of lactation secondary amenorrhoea • Chronic (adult): myxedema hypoadrenalism hair loss/depigmentation hypothermia hypoglycaemia • Chronic (childhood): proportional dwarfism Frolich’s syndrome
Microadenoma Anterior Pituitary • 1-5% of adults • Rarely have significant hormonal output
Effects of Pituitary Tumour • Hormone overproduction (e.g.TSH) with normal production of other hormones • Hormone overproduction with reduced production of other hormones • Pressure atrophy of gland with panhypopituitarism (non-functioning) • Space-occupying lesion in the skull
Clinically Significant Pituitary Tumours • Lactotroph 32.0% • Somatotroph 21.0% • Corticotroph 13.0% • Mixed somato/lacto 6.0% • Gonadotroph 1.0% • Thyrotroph 0.5% • Non-functional 26.5%
Syndromes of Common Functional Pituitary Adenomas • Lactotroph (PRL) Galactorrhoea Amenorrhoea • Somatotroph (GH) Acromegaly Gigantism • Corticotroph (ACTH) Cushing’s disease
Acromegaly: clinical features • Median age 30+. Equal male/female incidence. Characterised by acral enlargement, increased soft tissue mass, arthritis and osteoporosis. Diabetes develops in 30%. Serum GH elevated. • Possible compressive effects of tumour include visual field defects (bitemporal hemianopia), hypogonadism and amenorrhoea. • Tumours often display synthetic infidelity and may cause galactorrhoea, hyperpigmentation, hyperthyroidism, virilisation or adrenal hyperplasia • The condition of gigantism develops if epiphyses are unfused
Acromegaly Coarse facial features Big hands
Secondary Abnormalities of the Pituitary • “Feedback” tumours due to adrenal, thyroid or gonadal failure (Nelson-Salassa syndrome) • “Crooke’s hyaline change” in corticotrophs due to high plasma cortisol
Empty Sella Syndrome • The pituitary undergoes pressure atrophy due to a suprasellar mass compressing the gland in the sella turcica. • The pituitary becomes completely flattened, and clinical hypopituitarism accompanies this.
Diabetes Insipidus • Failure of ADH release from posterior pituitary due to destruction of hypothalamic-pituitary axons • Causes polyuria of up to 10L daily of low specific gravity urine with concomitant hypovolaemia and hypernatraemia • Urine specific gravity does not alter with fluid deprivation but increases with parenteral ADH
Cushing Disease/Syndrome • Cushing disease: overproduction of adrenal cortical glucocorticoids secondary to overstimulation by ACTH • Cushing syndrome: similar to Cushing disease, but is caused by adrenal cortical adenoma, adrenal cortical hyperplasia or adrenal cortical carcinoma
Cushing Disease • Moon face • Plethora
Advanced Cushing Disease • Truncal obesity • Buffalo hump • Wasting of extremities musclature
PINEAL GLAND • Pinecone shaped, minute, 180mg, at base of brain • Stroma and pineocytes (photosensory and neuroendocrine) • TUMOURS: • Germinomas, teratomas (sequestered germ cells) • Pinealomas (pineoblastoma, pineocytoma)
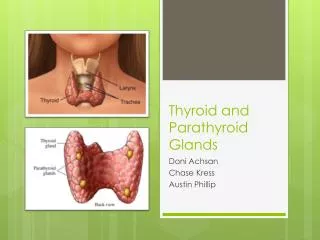
Normal Thyroid colloid
Thyroid Hormone Synthesis I- I2 + tyrosine Mono-iodotyrosine Di-iodotyrosine Triiodothyronine (T3) Thyroxine (T4)
Normal Thyroid Follicular epithelium
Thyroid Hormone Secretion • T3 (triiodothyronine) and T4 (thyroxine) are secreted into the rich vascular supply of the interstitium • The “C” cells of the interstitium secrete calcitonin which lowers serum calcium but has minimal functionality
Metabolic Effects of Thyroid Hormone 1. Uncouples oxidative phosphorylation a. less effective ATP synthesis b. greater heat release 2. Increases cardiac output, blood volume and systolic blood pressure 3. Increases gastrointestinal motility 4. Increases O2 consumption by muscle, leading to increased muscular activity with weakness
Thyroid Gland Development • Downward migration of epithelium from foramen caecum of tongue along the thyroglossal duct • Thyroglossal duct cysts develop from remnants of this path
Types of Thyroiditis • Lymphocytic (focal) :immunologic basis? • Hashimoto (struma lymphomatosa): antithyroid microsomal antibodies • Atrophic (primary myxedema): antithyroid microsomal antibodies • Granulomatous (de Quervain’s):mumps or adenoviral antibodies • Invasive fibrous (Riedel’s): unknown but associated with fibromatosis
Hashimoto Thyroiditis • Middle aged females. Diffuse rubbery goitre; initially painless, later atrophy • 50% hypothyroid at presentation, many euthyroid, minority hyperthyroid • All become hypothyroid eventually • Strong assn. with other autoimmune disease including SLE, RA, pernicious anaemia, Sjogren’s syndrome • Antibodies to TSH and thyroid peroxidases • Lymphocytic infiltration, Hurthle cell change, follicle destruction, replacement fibrosis
Hashimoto Thyroiditis-pathogenesis Abnormal T cell activation and B cell stimulation to secrete a variety of autoantibodies. Antibodies to TSH and thyroid peroxidases (antimicrosomal)
Hashimoto’s Thyroiditis Lymphoid follicle Hurthle cells
Hashimoto’s Thyroiditis Hurthle Cells