Download
1 / 34
350 likes | 674 Views
The Musculoskeletal system HIV and other infections. Johan van Rensburg. HIV AND THE MUSCULOSKELETAL SYSTEM. Important concepts in HIV and the musculoskeletal system. Concerning the HIV infection HIV modifies the presentation, clinical picture and outcome of auto-immune diseases

E N D
The Musculoskeletal system HIV and other infections Johan van Rensburg
Important concepts in HIV and the musculoskeletal system • Concerning the HIV infection • HIV modifies the presentation, clinical picture and outcome of auto-immune diseases • HIV infection may mimic many auto-immune diseases • Auto-antibodies may be present in both HIV (low titers) and auto-immune diseases • Considering immune suppression • HIV-virus more responsible for manifestations in early disease • Opportunistic infections and malignancies more prominent in late disease • Concerning the drugs • The drugs used to modify auto-immune disease may modify the outcome of HIV infection • HAART may present with musculoskeletal adverse events • Drug interactions must always be considered • Associated conditions • Same principles of diagnosis and management apply as in patient without HIV (after consideration of the above)
Musculoskeletal manifestations in HIV • More prevalent in late stages • Wide spectrum of disease • Prevalence uncertain • Quality of life influenced by pain, loss of function and systemic complications • Risk factors for HIV • Sexual history • IDU • Hemophiliacs
Examples of HIV and MS System Keep the normal course of HIV infection in mind
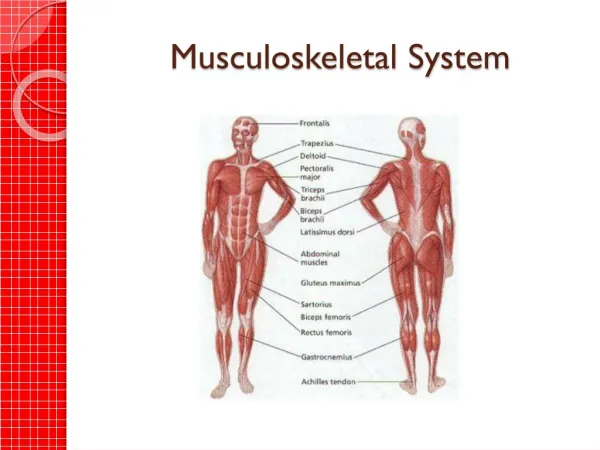
Remember • Components of the MS-system • Soft tissue • Muscles • Miopathy (virus and drugs), miositis (inflammatory or infective) • Ligamentsand enthesis • involved in reactive athritis and other sero-negative spondyloarthropathies • Blood vessels • Vasculitis, drug reactions and coagulopathies • Fat and other connective tissue • Involved in infection, drug reactions and crystal induced inflammation • Joints • Synovial joints • Infective: virus, septic arthritis, TB • Reactive • Auto-immune • Fibrous joints • Reactive athritis and other sero-negative spondyloarthropathies • Bone • Infections • Malignancies
POLYMYOSITIS (HIV MYOPATHY) • Any stage of HIV • Presents with • Bilateral proximal muscle weakness • Elevated CK levels • Pathogenesis uncertain • Diagnosis • Electromyography • MRI • Muscle biopsy • (Nerve conduction studies) • Treatment limited • HAART • Corticosteroids
PYOMYOSITiS • Advanced HIV • Presents with • Insidious muscle pain & swelling • With or without systemic symptoms • Requires prior muscle injury • Imaging • CT • MRI • Sonar • Treatment • Anti-microbials • Supportive • Surgery
NRTI MYOPATHY • Long term use • Dose-related mitochondrial toxicity • Prevalence 17% • Clinical picture • Similar presentation to polymyositis • Keep lactic acidosis in mind • Management • Discontinuation
ARTHRALGIA • Early disease • Acute HIV syndrome • Most patients seek medical attention • Fever, fatigue, maculopapular rash • 50-70% myalgias, arthralgias, paresthesias • Painful Articular Syndrome • 10% of HIV patients
ACUTE SYMMETRIC POLYARTHRITIS • Resembles rheumatoid arthritis • Characterized • Swan neck deformities • Ulnar deviation of the hand & digits • Radiographic results • Non erosive • Differentiation from RA • Atypical onset • RF usually negative (may be low positive with HIV) • Anti-CCP negative in HIV • Treatment • HAART • Symptomatic • Corticosteroids • Chloroquin
HIV ASSOCIATED ARTHROPATHY • Acute asymmetric oligoarthritis (Occurs late) • Resembles reactive arthritis • Presents • Acute severe pain • Large joints • 6 weeks to 6 months • Negative HLA B27 and RF • Treatment • HAART • Symptomatic • Corticosteroids
REITERS SYNDROME (Reactive arthritis) • Prevalence controversial 5-10% • Pathogenesis • HLA B27 positivity (more susceptible) • Clinical picture • “Incomplete” Reiter’s syndrome • Assymetrical arthritis and enthesopathies • Extra-articular manifestations • Treatment • HAART • Symptomatic • Corticosteroids • Salazopyrin
PSORIATIC ARTHROPATHY • Prevalence 3% • 10-40 X more frequent in HIV infected patients • Clinical picture • resembles psoriasis in the general population but may be more severe
HYPERTROPHIC OSTEOARTHROPATHY • Associated with • PCP • Bronchus Ca • Clinical picture • Severe pain in lower extremity • Clubbing • Arthralgias/periarticular soft tissue inflammation • Non-pitting oedema • Special investigations • Radiography • Periosteal reaction • Scintigraphy • Inflammation of distal ends of long bones • Treatment • Underlying cause
AVASCULAR NECROSIS • AVN and HAART • Possible link • HIV related risk factors • Corticosteroid • Megestrol • Hyperlipidemia • Pancreatitis • Non HIV related risk factors • Alcoholism • Hypercoagulability • Smoking • Common sites • Femoral head • Humeral head • Lunate (Kienbock disease) • Scaphoid (Preiser disease)
Musculoskeletal infections in HIV • Septic Arthritis • Tuberculosis Osteomyelitis • Bacillary Angiomatosis • Toxoplasmosis
Other conditions affecting the musculoskeletal system in HIV • Non-Hodgkin Lymphoma • Rhabdomyolysis • Myesthenia Gravis • Nemaline (Rod) myopathy • Fibromyalgia
Important concepts in HIV and the musculoskeletal system • Concerning the HIV infection • HIV modifies the presentation, clinical picture and outcome of auto-immune diseases • HIV infection may mimic many auto-immune diseases • Auto-antibodies may be present in both HIV (low titers) and auto-immune diseases • Considering immune suppression • HIV-virus more responsible for manifestations in early disease • Opportunistic infections and malignancies more prominent in late disease • Concerning the drugs • The drugs used to modify auto-immune disease may modify the outcome of HIV infection • HAART may present with musculoskeletal adverse events • Drug interactions must always be considered • Associated conditions • Same principles of diagnosis and management apply as in patient without HIV (after consideration of the above)
Principles for management • Musculoskeletal syndromes in HIV may be unrelated to HIV infection • Treat the underlying cause if possible • Rule out or correctly diagnosis infections • Probability of opportunistic infection depends on stage of HIV • Consider HIV related medications in differential diagnosis • High threshold when using immunosuppressive drugs
PitfallsSeptic Joint • Acute Monoarthritis is a rheumatologic emergency • Infection may destroy a joint in 48 hours
Septic Arthritis • Viral • Bacterial • Gram positive • Gram negative • Neiseria (GC, MC) • Anaerobic • Mycobacteria • Fungal
Septic Arthritis (Risk factors) • Immunosuppression (drugs, HIV) • Intravenous Drug Abuse • Abnormal joint (increased risk for septic arthritis) • OA • RA • Prosthesis • Remote infectious source
Patient with monoarticular complaint Careful exam reveals poliarticular arthritis Complete history and Physical examination Periarticular syndrome Tendinitis, bursitis, strain, sprain, osteomyelitis, soft tissue rheumatism True monoarticular arthritis Fracture, avulsion Acute changes Significant trauma or focal bone pain? Yes Radiograph Chronic changes OA, CPPD Effusion or inflammation? CBC, ESR, physical exam No Severe symptoms Yes Ultrasound-guided aspiration or CT/MRI Arthrocentesis
Arthrocentesis Synovial fluid WBC > 5000 Synovial fluid bloody Synovial fluid WBC < 1000 Acute inflammatory arthritis Non-inflammatory arthritis (OA, internal derangement) MRI Arthroscopy Occult fracture, tumor, internal derangement Internal derangement
Acute inflammatory arthritis (synovial fluid WBC > 5000/cm3) + Gram stain Infection _ Young: GC > staph >strep Old: staph > strep > GC Immunocompromised: Staph, gram-negative, other unusual organisms + Gout, CPPD r/o superinfection Crystal exam - CBC, ESR, RF, ANA, Ricketsae + Empiric antibiotics x24 hours, awaiting cultures - + Systemic toxicity? CPPD, reactive arthritis, systemic rheumatic disease Anti-inflammatory medication; Follow-up in 24-48 hours; Re-aspirate joint if worsens
Infected joint in RA Back
TUBERCULOSIS Pott’s disease Involvement of bone and discs with collapse of vertebrae
TUBERCULOSIS Monoarthritis and Tendosynovitis Destructive joint disease Monitor for extra-articular TB