Download
1 / 20

E N D
1. Principles of Casting and Splinting Naomi N. Shields, M.D.
February 8, 2012
2. Introduction Casts and splints
Immobilize
Position
Protect
Used for
Fractures
Sprains
Soft tissue and crush injuries
3. Workshop Brief overview
Demonstration of Short arm cast or splint
Demonstration of cast removal
Hands on�don�t forget to remove them from your friends!
4. Principles of Application Avoid wrinkles
Even layer cast padding
Overlap by �
Wrap distal to proximal
Avoid tourniquet effect
5. Principles of Application Use palms/flat of hand to mold
Avoid fingertips
Creates indents and cast sores
Rubbing cast well (esp plaster) laminates
Avoid burns
Hotter water and more layers cast material = HEAT as cast sets up
Be careful with young, elderly or insensate pt
6. Supplies Stockinette
2-6� sizes
Cut or fold at ankle, elbow, knee to avoid wrinkle
Roll up to roll on
Synthetic or cotton
7. Supplies Cast padding
Synthetic
Cotton
Gortex
Cast material
Plaster
Fiberglass
Polyester
Splint material
Plaster
Fiberglass (OCL, etc)
8. Common UE Splints Volar or short arm
Radial Gutter
Ulna Gutter
Thumb spica
Sugar Tong
Long arm
Commonly used after injury to allow swelling
Often utilized after surgery
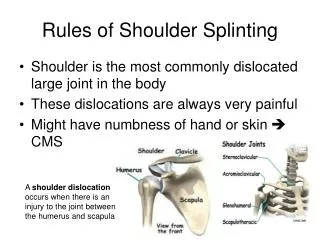
9. Upper Extremity Splints Pt positioning
Supine with shoulder abducted, elbow flexed (hold digits), control forearm rotation
Sitting with elbow resting table, thumb and fingers towards ceiling (gives slight dorsal flexion to wrist) Thumb spica
Thumb and index in apposition
Gutter splints
MCP�s FLEXION
PIP/DIP�s EXTENSION
If reverse VERY difficult to get motion back in digits
10. Application UE splints Position patient
Wrap with webril (2-3�)
Apply splint material
Overwrap with kling or kerlix
Apply Ace
Mold/Hold til set up Avoid bulk through anterior elbow (especially fractures near elbow � may impair circulation!)
Figure 8 wrap at elbow effective
11. Comments re Sugar Tong Controls forearm rotation better then Short arm
Keep volar and dorsal edges apart � if touch mid forearm create circumfrential tourniquet For better elbow immobilization � one sugar tong from palm around elbow to dorsum hand � second from axilla around elbow to back of arm
12. UE Casts Short arm cast (SAC)
Long arm cast (LAC)
Munster
Thumb spica
13. Common LE Splints Posterior Splint
Posterior with Stirrup
Short Leg Compression
Long Leg
Knee Immobilizer Applications steps like UE
May be helpful to position pt prone (esp if heavy pt)
Long leg may need reinforcement at knee
14. Common LE Casts Short Leg (SLC)
Short Leg Walking (SLWC)
Patella Tendon Bearing
Long Leg (LLC)
Total Contact Cast
Cylinder
15. Cast Application Position Patient
Apply Stockinette
16. Cast Application In UE casts
follow palmar crease for hand function
Appose thumb + index
In LE casts
Don�t get too high into popiteal fossa short leg
Consider great and little toes
17. Cast Removal Cast saw vibrates
Can CUT skin IF dragged
Support saw with hand
Go down throught material then come back up and move in direction of cut out of cast � go back down Use spreader to separate cast
Bivalve vs univalve
Use scissors to cut around top and bottom of top shell to remove
Cut longitudinal through stockinette/padding
Saw Blade MAY get hot!
18. Cast Complications To tight = PAIN possible compartment syndrome
Univalve or bivalve
Pressure sores
Due to pressure
Due to rubbing if loose
Skin maceration or fungus
19. Cast Complications Cast Breakdown
Under heel � too much padding or not enough material
Can crack at junction rolls if rolls not taken full length of cast
Cast malposition
Loosening
If limb swollen when applied, will often need to change 3-7 days later
Wet/Damp cast
From bathing
From sweat
20. Summary Hand out includes cast care guidelines
Good idea to give written handout to patients!
Also includes some tips on casting in general as well as guidance for various casts
It takes time and practice to become proficient at casting. If a patient comes in with a problem cast, evaluate it to see what went wrong, what could be done differently and use these casts to further educate yourself. Now on to hands on��.