Download
1 / 25
320 likes | 1.4k Views
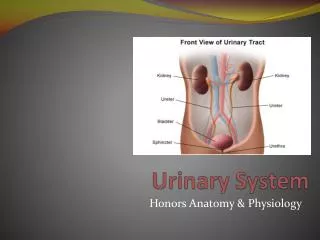
Structures and Functions of the Urinary System. Please review your A

E N D
1. Nursing Assessment: Urinary System NURS 1228
Spring 2003
By Nina Green, RN, Instructor
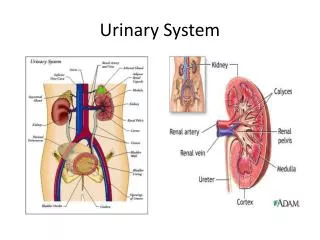
2. Structures and Functions of the Urinary System Please review your A & P textbook
Look closely at the Macrostructure and Microstructure of the Kidneys
3. Normal Glomerular Filtrate (Review) Normally the capillary pores are to small to allow loss of large blood components.
With many renal diseases, capillary permeability is increased allowing plasma proteins to enter urine.
It is like blood, except it doesn�t have the large blood components (plasma proteins, blood cells, and platelets)
4. Normal Glomerular Filtration Rate Normal GFR is 125 ml/minute
However, because much is reabsorbed by the peritubular capillary network as the filtrate travels toward the collecting duct, usually only 1 ml/minute is excreted as urine
5. Antidiuretic Hormone (ADH) Released from the posterior pituitary gland
Stimulated by increased serum osmolality and decreased blood volume
Acts on the distal convoluted tubules and collecting ducts increasing wall permeability to water, allowing water reabsorption back into the capillaries.
6. Aldosterone Released from the adrenal cortex
Release is stimulated by the circulating blood volume and plasma concentrations of sodium ion (Na+) and potassium ion (K+)
Acts on the distal tubule
Causes the reabsorption of (Na+) and water.
In exchange for Na+, K+ is excreted.
7. Acid-base regulation The conservation of bicarbonate (HCO3-) and the excreting of excess hydrogen ion (H-).
The distal tubule functions to maintain the pH of the ECF between 7.35 and 7.45
8. Atrial Natriuretic Factor (ANF) Hormone released from the right atrium of heart
Stimulated by elevated right atrial blood pressures
Inhibits secretion of ADH and its effect on reabsorption of water into blood system
Causes dilute urine in large amounts
9. Parathyroid Hormone Released from the parathyroid gland
Stimulated by low serum calcium (Ca++) levels in blood
Causes the reabsorption of calcium ions increasing serum calcium
10. Other Renal Functions Production of erythropoietin
Released in response to decreased oxygen tension in the renal blood supply (usually due to loss of RBC�s)
Stimulates the production of RBC�s in bone marrow
A deficiency of erythropoietin causes anemia in renal failure
11. Other Renal Functions Assists in the activation of Vitamin D
Ingested Vitamin D and Vitamin D from the sun via the skin are inactive until they are acted upon by the liver and kidney.
Vitamin D is essential for the uptake of calcium from the GI tract.
The patient with renal failure has a deficiency of the active metabolite Vitamin D and so has problems with calcium and phosphate balance.
12. Other Renal Functions Renin
Assists in the regulation of blood pressure
Is released in response to decreased arterial blood pressure,renal ischemia, ECF depletion, increased norepinephrine, and increased levels of Na+ in urine
Catalyzes the splitting of the plasma protein angiotensinogen into angiotensin 1
13. Other Renal Functions Angiotension 2
Is converted from angiotension 1
Stimulates the release of aldosterone. (Na+ and water retention and yields greater ECF volume)
Causes increased peripheral vasoconstriction which combined with the increased ECF volume causes increased blood pressure. This inhibits the release of renin.
14. Prostaglandin's Synthesized by most body tissues
In kidney, produced mainly in Medulla
Causes vasodilation, increased blood flow, and Na+ excretion, lowers blood pressure
Counteracts angiotensin and norepinephrine
Loss of Prostaglandin tissue in the kidney due to renal failure ? Cause of HTN in renal patients.
15. Organs of Urinary System Kidneys
Ureters
Urethra
Female 1-2 inches long
Male 8-10 inches long
Meatus* Bladder
Urethrovesical Unit
Bladder
Bladder neck
Urethra
Pelvic floor muscles Meatus is not mentioned in text, but it is included because it is included when discussing cancers.Meatus is not mentioned in text, but it is included because it is included when discussing cancers.
16. Effects of aging on Urinary System Decreased
Renal tissue
Number of nephrons
Renal vascular supply
Function of loop of Henle and tubules
Elasticity of muscle tone in bladder/urethra Decreased
Bladder capacity and sensory receptors
Weakened
Urinary sphincter
Estrogen deficiency causing thin, dry vaginal tissues
Prostatic enlargement Between ages 30-90 there is a 20-30% decrease in the size and weight of the kidneys
By age 70 about 30-50% of glomeruli have lost their function. Blood flow to the kidney decreases.
This causes a decreased glomerular filtration rate (GFR) and a reduced ability of the glomeruli and tubules to conserve Na+, dilute or concentrate urine, and excrete acid load, and etc�.
Decreased estrogen levels in older women causes urethral irritation, urethral and bladder infections, and urinary incontinence.
In men, the prostate enlarges with age and can affect urination. May cause a partial obstruction.
Constipation can affect urination also.Between ages 30-90 there is a 20-30% decrease in the size and weight of the kidneys
By age 70 about 30-50% of glomeruli have lost their function. Blood flow to the kidney decreases.
This causes a decreased glomerular filtration rate (GFR) and a reduced ability of the glomeruli and tubules to conserve Na+, dilute or concentrate urine, and excrete acid load, and etc�.
Decreased estrogen levels in older women causes urethral irritation, urethral and bladder infections, and urinary incontinence.
In men, the prostate enlarges with age and can affect urination. May cause a partial obstruction.
Constipation can affect urination also.
17. Causing Kidneys to be less palpable
Decrease in creatinine clearance, increase in BUN
Alterations in drug excretion
Nocturia, frequency, urgency, incontinence Decreased ability to concentrate urine, diluted urine
Loss of usual pattern with urination
Urine retention
Stress incontinence, dysuria, dribbling
Increased infections
18. Functional Health Patterns Health Perception-Health Management Pattern
How is energy level?
Vision changes?
Smoker? How long? Nutritional-Metabolic Pattern:
How is appetite?
Weight changes?
Vitamin or mineral supplements?
Kinds of fluids drink? How much? Caffeine?
Caffeine or spicy foods? How much?
19. Functional Health Patterns Elimination Pattern
Urination, how often? Nocturia?
Color? Blood?
Urgency? Frequency? Incontinence? Dribbling? Pain?
Use special devices for elimination or control?
Bowels regular? Activity-Exercise Pattern
Changes in ADL�s?
Activities aggravate urinary problem?
Urinary problem caused you to alter or stop activities or exercise?
Require assistance moving? To bathroom?
20. Functional Health Patterns Cognitive-Perceptual Pattern
Pain with urination? Self-Perception-Self-Concept Pattern
How does urinary problem make you feel about yourself?
Different body perception since urinary problem?
21. Functional Health Patterns Role-Relationship Pattern
Problems with relationships due to urinary problem?
Change in job status or ability to do job related responsibilities due to urinary problem? Sexuality-Reproductive Pattern
Change in sexual pleasure or performance due to urinary problem?
Hygiene problems r/t sexual activities causing concerns?
22. Functional Health Patterns Coping-Stress Tolerance Pattern
Able to manage urinary problem?
Strategies using to cope with urinary problem? Values-Beliefs Pattern
Present illness affecting belief system?
Treatment decisions r/t urinary problem in conflict with value system?
23. Common Abnormalities of Urinary System Dysuria
Frequency
Enuresis
Hesitancy
Urgency
Hematuria
Burning on urination
Pneumaturia Retention
Pain
Incontinence
Stress incontinence
Nocturia
Polyuria
Anuria
Oliguria
See text pg 1250 Table 42-7See text pg 1250 Table 42-7
24. Diagnostic Studies of the Urinary System Urine Studies
Urinalysis
Creatinine clearance
Urine culture (clean catch midstream)
Concentration test
Residual urine
Protein determination
Urine cytology Blood Chemistries
BUN
Creatinine
Uric acid
Sodium
Potassium
Calcium
Phosphorus
bicarbonate BUN Blood urea nitrogen is a by product of the breakdown of amino acids used for energy production. It is a rough indicator of decreased kidney function. It is elevated in kidney failure, shock, GI bleeding, diabetes and some tumors. Normal range is 10-30mg/dl. Increase may mean renal problems.
Creatinine The decomposition product of the metabolism of phosphocreatine, a source of energy for muscle contraction. Increased quantities of it are found in advanced stages of renal disease. It is a normal alkaline constituent of urine and blood. Normal serum range is 0.5-1.5mg/dl.
BUN/Creatinine ratio normal finding is 10:1
Uric acid normal finding is 2.5-5.5mg/dl for women and 4.5-6.5mg/dl for men
Sodium normal range is 135-145mEq/l
Potassium normal range is 3.5-5.5mEq/l
Calcium normal range is 9-11mg/dl
Phosphorus normal range is 2.8-4.5 mg/dl
Bicarbonate normal range 20-30mEq/l. Most patients in renal failure have metabolic acidosis and low serum HCO3- levels.BUN Blood urea nitrogen is a by product of the breakdown of amino acids used for energy production. It is a rough indicator of decreased kidney function. It is elevated in kidney failure, shock, GI bleeding, diabetes and some tumors. Normal range is 10-30mg/dl. Increase may mean renal problems.
Creatinine The decomposition product of the metabolism of phosphocreatine, a source of energy for muscle contraction. Increased quantities of it are found in advanced stages of renal disease. It is a normal alkaline constituent of urine and blood. Normal serum range is 0.5-1.5mg/dl.
BUN/Creatinine ratio normal finding is 10:1
Uric acid normal finding is 2.5-5.5mg/dl for women and 4.5-6.5mg/dl for men
Sodium normal range is 135-145mEq/l
Potassium normal range is 3.5-5.5mEq/l
Calcium normal range is 9-11mg/dl
Phosphorus normal range is 2.8-4.5 mg/dl
Bicarbonate normal range 20-30mEq/l. Most patients in renal failure have metabolic acidosis and low serum HCO3- levels.
25. Diagnostic Studies of the Urinary System Radiologic Procedures
Kidneys, ureters, bladder (KUB)
IVP or excretory urogram
Nephrotomogram
Retrograde pyelogram
Radiologic Procedures
Cystogram
Renal arteriogram (angiogram)
Ultrasound
CT scan
MRI KUB is a flat abdominal x-ray taken without contrast to show the renal outline, surrounding musculature and the bladder if it is full. Stones and foreign bodies (tumors) can be seen with this x-ray.
IVP or excretory urogram, is to visualize the urinary tract. Gives clues to renal function. Uses IV contrast material, which circulates in the blood and is excreted in the kidneys and urinary tract. Is possible to detect tumors, cysts, lesions, and obstructions.
Nephrotomogram is similar to a CT scan. An IV contrast is given and excreted in the kidneys. Pictures are taken of the kidneys during the procedure in sections. Can see blockages, stenosing and other factors causing urinary problems.
Retrograde pyelogram is similar to an IVP. Contrast is inserted directly into the kidney and pictures are taken sequentially. Contrast is inserted via a urinary catheter inserted through a cystoscope. There is a risk of infection and patient undergoes sedation. Is used if patient is allergic to contrast media, has decreased renal function or IVP was inconclusive in findings.
Cystogram: contrast media is instilled into bladder via a cystoscope or urinary catheter. Purpose is to visualize the bladder and evaluate for reflux of urine.
Renal arteriogram: contrast material is injected into the renal artery via a catheter inserted into the femoral artery. Purpose is to visualize the renal blood vessels.
Ultrasound is a noninvasive procedure ulilizing sound waves inserted into body structures and recorded. A computer interprets the tissue density based on sound waves and displays it in a picture form.
CT scan provides excellent visualization of kidneys. Advantage over ultrasound is that the CT scan can pick up subtle differences. IV contrast media is given. Tumors and abnormalities can be detected easily.
MRI is computer generated films that rely on radio waves and alteration in magnetic field. Not useful in detecting some tumors and foreign bodies. Used to visualize the kidneys.KUB is a flat abdominal x-ray taken without contrast to show the renal outline, surrounding musculature and the bladder if it is full. Stones and foreign bodies (tumors) can be seen with this x-ray.
IVP or excretory urogram, is to visualize the urinary tract. Gives clues to renal function. Uses IV contrast material, which circulates in the blood and is excreted in the kidneys and urinary tract. Is possible to detect tumors, cysts, lesions, and obstructions.
Nephrotomogram is similar to a CT scan. An IV contrast is given and excreted in the kidneys. Pictures are taken of the kidneys during the procedure in sections. Can see blockages, stenosing and other factors causing urinary problems.
Retrograde pyelogram is similar to an IVP. Contrast is inserted directly into the kidney and pictures are taken sequentially. Contrast is inserted via a urinary catheter inserted through a cystoscope. There is a risk of infection and patient undergoes sedation. Is used if patient is allergic to contrast media, has decreased renal function or IVP was inconclusive in findings.
Cystogram: contrast media is instilled into bladder via a cystoscope or urinary catheter. Purpose is to visualize the bladder and evaluate for reflux of urine.
Renal arteriogram: contrast material is injected into the renal artery via a catheter inserted into the femoral artery. Purpose is to visualize the renal blood vessels.
Ultrasound is a noninvasive procedure ulilizing sound waves inserted into body structures and recorded. A computer interprets the tissue density based on sound waves and displays it in a picture form.
CT scan provides excellent visualization of kidneys. Advantage over ultrasound is that the CT scan can pick up subtle differences. IV contrast media is given. Tumors and abnormalities can be detected easily.
MRI is computer generated films that rely on radio waves and alteration in magnetic field. Not useful in detecting some tumors and foreign bodies. Used to visualize the kidneys.
26. Diagnostic Studies of the Urinary System Renal Radionuclide Imaging
Renal Scan
Endoscopy
Cystoscopy
Urodynamics
Cystometrogram
Invasive Procedure
Renal biopsy Renal Scan Radioactive isotopes are injected IV. Radiation detector probes are placed over kidney, and scintillation counter monitors radioactive material in kidney. Purpose is to show blood flow, glomerular filtration, tubular function, and excretion. The radioisotope distribution in the kidney is scanned and mapped.
Cystoscopy: study involves use of tubular lited scope to inspect the bladder. Is done under local or general anesthesia.
Cystometrogram: is a study where a catheter is inserted and water or saline is instilled into the bladder. Measurements are taken of the pressure this exherts on the bladder wall. Purpose is to evaluate bladder tone, sensations of filling, and bladder stability.
Renal Biopsy: is usually done as a skin biopsy through needle insertion into the lower lobe of the kidney. The purpose is obtain renal tissue for examination to determine type of renal disease or to follow the progress of renal disease.
Renal Scan Radioactive isotopes are injected IV. Radiation detector probes are placed over kidney, and scintillation counter monitors radioactive material in kidney. Purpose is to show blood flow, glomerular filtration, tubular function, and excretion. The radioisotope distribution in the kidney is scanned and mapped.
Cystoscopy: study involves use of tubular lited scope to inspect the bladder. Is done under local or general anesthesia.
Cystometrogram: is a study where a catheter is inserted and water or saline is instilled into the bladder. Measurements are taken of the pressure this exherts on the bladder wall. Purpose is to evaluate bladder tone, sensations of filling, and bladder stability.
Renal Biopsy: is usually done as a skin biopsy through needle insertion into the lower lobe of the kidney. The purpose is obtain renal tissue for examination to determine type of renal disease or to follow the progress of renal disease.