Download
1 / 25
260 likes | 544 Views
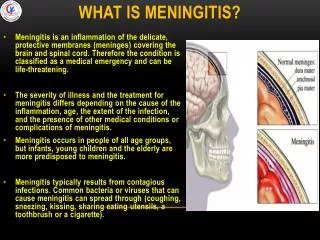
MENINGOCOCCAL MENINGITIS (MCM) AT DELHI & INDIA. Dr. A. K. AVASARALA MBBS, M.D. PROFESSOR & HEAD DEPT OF COMMUNITY MEDICINE & EPIDEMIOLOGY PRATHIMA INSTITUTE OF MEDICAL SCIENCES, KARIMNAGAR, A.P. INDIA: +91505417 avasarala@yahoo.com. PART - I MCM PROBLEM AT DELHI

E N D
MENINGOCOCCAL MENINGITIS (MCM) AT DELHI & INDIA Dr. A. K. AVASARALA MBBS, M.D. PROFESSOR & HEAD DEPT OF COMMUNITY MEDICINE & EPIDEMIOLOGY PRATHIMA INSTITUTE OF MEDICAL SCIENCES, KARIMNAGAR, A.P. INDIA: +91505417 avasarala@yahoo.com
PART - I • MCM PROBLEM AT DELHI AND REST OF INDIA
PROMPT • THIS JUST IN TIME (JIT) LECTURE IS DEVELOPED AS DELHI IS SUFFERING FROM 405 CASES AND 48 DEATHS DUE TO MCM. (AS ON JUNE 14TH 2005) • MCM IS NOT NEW FOR DELHI. SINCE 1966, DELHI IS FACING THE BRUNT OF REPEATED EPIDEMICS OF MCM. • WHY? IS DELHI BECOMING A HOME TOWN FOR MCM? • THIS AROUSED INTEREST IN ME TO DEVELOP THIS JIT LECTURE.
LEARNING OBJECTIVES • LEARNER SHOULD KNOW THE ENTIRE NATURAL HISTORY OF THE DISEASE • LEARNER SHOULD UNDERSTAND MCM PROBLEM IN DELHI AND IN REST OF INDIA • HE SHOULD LEARN THE STRATEGIES TO CONTROL MCM • HE SHOULD BE ABLE TO ANALYZE AND DISCUSS THE SITUATION
PERFORMANCE OBJECTIVES • LEARNER CAN APPLY THIS KNOWLEDGE AND CONTROL STRATEGIES TO OTHER INFECTIOUS DISEASES OF SAME BEHAVIOUR.
DELHI 1966 FEATURES • TOTAL CASES 616, MOSTLY MALE INFANTS • ADMITTED IN 5 MAJOR HOSPITALS IN DELHI • SEROGROUP NOT DETERMINED • INCREASE IN PROPORTION OF LABORATORY CONFIRMED CASES FROM 4.8% IN JANUARY 10.6% IN FEB 44.9% IN MAY
DELHI 1985 FEATURES • LARGE EPIDEMIC AFTER 20 YEARS GAP , • TOTAL CASES 6133 • DEATHS 799 • CASE FATALITY RATE 13%
PRESENT EPIDEMIC AT DELHI DEATHS (cumulative total & CASE FATALITY RATE) DURATION CASES 42 DAYS 29-3-2005 TO 9-5-2005 187 15 ONE WEEK 9-5-2005 TO 16-5-2005 116 26 (8.6%) JUST 2 DAYS 16TH TO 18 TH MAY 2005 10 26 JUST 12 DAYS (18-05-2005 TO 30-5-2005) 55 37 37 48 From 30-5-05 to 8-6-05 Total as on 14-6-05 405 48 (10.9%)
DELHI EPIDEMIC 2005 Deaths Cases
AGE & SEX DISTRIBUTION OF CASES & DEATHS • MORE CASES (44%) AND MORE DEATHS (62%) IN 15-29 YEARS GROUP AGE GROUP <5 YEARS +6% AGE GROUP 5-14 =32% AGE GROUP 15-19=44% AGE GROUP 30-44=10% AGE GROUP 45+ =6% SEX PREDILICTION =M:F= 74%: 26% • CASES SEX DISTRIBUTION -M:F=74:26
SERO GROUP TYPING • PRESENT EPIDEMIC IS DUE TO SEROTYPE ” A” MENINGOCOCCI
PLACE DISTRIBUTION PLACES AFFECTED ARE MOSTLY OVERCROWDED: • CITY, • SHAHDARA NORTH, • SADAR PAHAR GANJ, • SHAHDARA SOUTH, • CIVIL LINES, • CENTRAL DELHI
ACTION PLAN • SECRETARY LEVEL (HEALTH) MEETING • DIRECTOR GENERAL HEALTH SERVICES TECHNICAL INCHARGE AND DAILY MONITORING • WHO TECHNICAL ASSISTANCE • COORDINATION & EXPERTS COMMITEE • PUBLIC EDUCATION • SURVEILLANCE • RISK COMMUNICATION • MEDIA BRIEFS
CONTROL MEASURES TAKEN • DIAGNOSIS AND TREATMENT OF ALL CASES • CONTACT TRACING OF ALL CLINICALLY SUSPECT CASES • CHEMO PROPHYLAXIS FOR 305 HOUSE-HOLDS • 12000 VACCINATIONS OF QUADRIVALENT MENINGO COCCAL VACCINE • 35 CSF SAMPLES TESTED +VE FOR TYPE”A’ MENINGOCOCCI • RISK COMMUNICATION
INITIAL LETHARGY IN FIRST 42 DAYS OF EPIDEMIC 2005 • FROM MARCH 29-3-2005 TO 9-5-2005, (42 DAYS) 187 CASES ARE ALLOWED TO ACCUMULATE. WHY? ( on average almost 4-5 cases per day) • IS IT DUE TO DELAYED INITIATION OF ACTION? • IS IT DUE TO DELAYED NOTIFICATION? • IS IT DUE TO DELAYED CASE FINDING? • OR REDUNNDANCY OT THE PART OF HEALTH AUTHORITIES AS MCM EPIDEMICS ARE COMMON TO DELHI
THREE FOLD DAILY INCREASE 2005 • NEXT WEEK ANOTHER 116 CASES (16 CASES/DAY) CLEARLY INDICATES THAT ACTION INITIATED IS NOT ADEQUATE OR PROPER. • IS THE STRATEGY WRONG OR IS IT DUE TO INSUFFICIENT OR INEFFICIENT APPLICATION OF CONTROL MEASURES.
OTHER INDIAN STATES AFFECTED IN 1985 • HARYANA (FARIDABAD, GURGAON, ROTHAK) • UTTAR PRADESH (GHAZIABAD, AGRA, MATHURA, ALIGARH, MUZAFFARNAGAR, BULANDSHAHAR, MEERUT) • RAJASTHAN (BHARATPUR, JAIPUR, BIKANEER) • SIKKIM (GANGTOK) • GUJARAT • JAMMU&KASHMIR • WEST BENGAL(CALCUTTA) • KERALA • ORISSA
OTHER INDIAN STATES AFFECTED IN 1989 • MADHYA PRADESH • ORISSA • ANDHRA PRADESH
1989 MADHYA PRADESH FEATURES • TOTAL CASES =249 (AS ON 20-3-1989) • DEATHS = 67 • MENINGO COCCUS TYPE “A” OUTBREAK • IN DISTRICTS OF SAGAR, DAMOH, CHATTARPUR, MANDSAUR, UJJAIN, SATNA, SHAHJAHANPUR, INDORE 1989 ORISSA FEATURES • CASES = 2951 • DEATHS = 344 • DISTRICTS AFFECTED: KALAHANDI, KOHLAPUR, PHULBANI
1989 ANDHRA PRADESH FEATURES • TOTAL CASES = 475 • TOTAL DEATHS = 108 • MENIGOCOCCAL TYPE “A” EPIDEMIC • DISTRICTS OF VISAKHAPATNAM, VIJAYANAGARAM, SRIKAKULAM
1989 PERSONAL EXPERIENCE - 1 WE HAVE VISITTED A RESIDENTIAL SCHOOL AT PACHIPENTA, VIZIANAGARAM DISTRICT TO SEE FOUR BOYS BEDRIDEN WITH FEVER, HEADACHE, NECK STIFFNESS AND TYPICAL PETICHIAL RASH SKIN RASHES 42 BOYS ARE LIVING IN THAT OVERCROWDED HALL
PERSONAL EXPERIENCE - 2 • ON INVESTIGATION, WE DIAGNOSED IT AS MCM AND FOUND THAT TWO CASES PER YEAR HAVE OCCURRED IN THE PAST TWO YEARS REVEALING ITS USUAL SPORADIC INITIATION • 1989 EPIDEMIC INVOLVED NEIGHBOURING DISTRICTS OF VISAKHAPATNAM, AND SRIKAKULAM RESULTING IN 475 CASES AND 108 DEATHS