Download
1 / 29
320 likes | 870 Views
Approach to Acute Monoarthritis of the Knee. Henry Averns Assistant Professor Rheumatology Division Queens University. Aims of Workshop. To consider the differential diagnosis of acute and chronic knee monoarthritis

E N D
Approach to Acute Monoarthritis of the Knee Henry Averns Assistant Professor Rheumatology Division Queens University
Aims of Workshop • To consider the differential diagnosis of acute and chronic knee monoarthritis • I.e. provide a systematic approach to the investigation and differential diagnosis of patients presenting with monoarticular pain. • To briefly review examination of the knee • To discuss indications for aspiration and injection of the knee • To practice knee injection on model knees
APPROACH TO MONOARTHRITIS OF THE KNEE MONOARTHRITIS POLYARTHRITIS Acute or Chronic? Is it inflammatory? Extra- articular features? Systemic or local problem? ARTICULAR EXTRA-ARTICULAR
History I • Age, time profile • Features of inflammation • stiffness, redness, pain, swelling, warmth • Preceding illness • GU or GI infection • history of trauma, portal of entry for infection • Associated symptoms • red eye, rash, balanitis
History 2 • Associated medical complaints • psoriasis, IBD, Ankylosing spondylitis • bleeding disorders • predisposition to infection • Drug history • immunosuppressants, aspirin, diuretics • Family history • of gout, psoriasis, IBD, AS
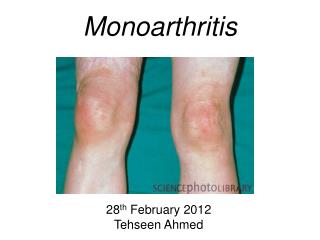
Differential diagnosis I • Acute monoarthritis • Septic arthritis (staph aureus) • Reactive arthritis • GI infection - campylobacter, salmonella, shigella, yersinia • GU infection - chlamydia • Crystal arthritis • Gout (uric acid) • Pseudogout/chondrocalcinosis/calcium pyrophosphate deposition disease (CPPD) • Haemarthrosis
Septic Arthritis • Risk factors • prosthetic hip or knee joint, • skin infection, • joint surgery, • rheumatoid arthritis, • age greater than 80 years, • diabetes mellitus. • Intravenous drug use and large-vein catheterization are predisposing factors for sepsis in unusual joints (e.g., sternoclavicular joint).
Examination of the Knee • Demonstration • Module
ARTHROCENTESIS / INJECTION • Indications • Diagnostic • Synovial fluid analysis • Therapeutic • Inflammatory arthritis • Gout • Osteoarthritis
ARTHROCENTESIS The things you need;
ARTHROCENTESIS • Contraindications • Infection locally OR elsewhere • Abnormal skin (relative CI) • Warfarin therapy is not a contraindication • No touch technique adequate • Local anaesthesia difficult to achieve…is it worth it? Probably not • Have appropriate tubes ready
Extra-articular features which suggest seronegative spondyloarthritis • nails (pitting, ridging, hyperkeratosis) • enthesitis, dactylitis and tenosynovitis • nodules (elbows/ears) • skin (local infection, psoriasis, keratoderma blenorrhagicum, balanitis) • eyes (conjunctivitis, uveitis) • mouth ulcers
Investigations I • Haematology - CBC, ESR, clotting • Biochemistry - U&E, LFTs, urate, CRP • Immunology • Microbiology • blood/urine/stool/urethral/sputum cultures • serology
Investigations II • Synovial fluid • volume/viscosity/cellularity • polarised light microscopy (crystals) • gram stain/culture • Imaging • plain films • loss of joint space, osteophytes, subchondral cysts, osteosclerosis, erosions, chondrocalcinosis • MRI, bone scan
Septic Arthritis • Staph aureus—most common • Strep (splenic dysfunction) • Neisseria gonorrhea (young, sexually active) • Gram negatives (immunocompromised, GI infection) • Mycobacteria (immunocompromised) • Fungus (immunocompromised) • Lyme disease