Download
1 / 9
90 likes | 352 Views
Radiation Dose in MS - CT coronarography. Ladislav Pavic, MD, PhD Sunce Clinics Zagreb / Sarajevo Croatia / Bosnia & Herzegovina. Introduction. With 64 ≥ slice CT scaners, CCTA has emerged as a useful diagnostic imaging modality for the assessment of coronary artery disease.

E N D
Radiation Dose in MS-CT coronarography Ladislav Pavic, MD, PhD Sunce Clinics Zagreb / Sarajevo Croatia / Bosnia & Herzegovina
Introduction With 64 ≥ slice CT scaners, CCTA has emerged as a useful diagnostic imaging modality for the assessment of coronary artery disease. It is considered appropriate for selected indications: patients with a low-to-intermediate pretest probability for obstructive CAD rapid evaluation of patients with chest pain in emergency by-pass analysis etc. The clinical usefulness of CCTA has to be weighed against the radiationexposure and the smallbut potential risk of cancer induction! ACCF/ACR/SCCT/SCMR/ASNC/NASCI/SCAI/SIR 2006 appropriateness criteria for cardiac computed tomography and cardiac magnetic resonance imaging: a report of the American College of Cardiology Foundation Quality Strategic Directions Committee Appropriateness Criteria Working Group, American College of Radiology, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, American Society of Nuclear Cardiology, North American Society for Cardiac Imaging, Society for Cardiovascular Angiography and Interventions, and Society of Interventional Radiology. Hendel RC, et al. J Am Coll Cardiol. 2006;48:1475-1497.
Introduction Computed tomography represents animportant source of ionizing radiationarising from medical exposures Since the inception of CT in the 1970s, its use has increased rapidly. It is estimated that more than 62 million CT scans per year are currently obtained in the US Small series reported CCTA radiationdoses of up to 21.4 mSv without useof electrocardiographically controlled tube current modulation Othersmall series reported radiationdoses as low as 2.1 mSv with the applicationof newly available sequentialscanning algorithms. Although the risks for any one person are not large, the increasing exposure to radiation in the population may be a public health issue in the future. Gerber TC, et al. Ionizing radiation in cardiac imaging: a science advisory from the American Heart Association Committee on Cardiac Imaging of the Council on Clinical Cardiology and Committee on Cardiovascular Imaging and Intervention of the Council on Cardiovascular Radiology and Intervention. Circulation. 2009 Feb 24;119(7):1056-65. Epub 2009 Feb 2.
Measuring radiation - Dosimetry Effective dose (E, SI units - mSv): reflects the risk of the biological effects of ionizing radiation, represents the amount of whole-body irradiation that would yield a biological risk equivalent to that of an irradiation to only a portion of the body, such as that which occurs during a diagnostic or therapeutic medical procedure, is useful in comparisons of the biological risk of different medical procedures that use ionizing radiation, given the uncertainties regarding organ risk and the inability of E to reflect individual patient risk, differences between estimates of the E by a factor of less than 2 cannot be considered significant Gerber TC, et al. Ionizing radiation in cardiac imaging: a science advisory from the American Heart Association Committee on Cardiac Imaging of the Council on Clinical Cardiology and Committee on Cardiovascular Imaging and Intervention of the Council on Cardiovascular Radiology and Intervention. Circulation. 2009 Feb 24;119(7):1056-65. Epub 2009 Feb 2.
Gerber TC, et al. Ionizing radiation in cardiac imaging: a science advisory from the American Heart Association Committee on Cardiac Imaging of the Council on Clinical Cardiology and Committee on Cardiovascular Imaging and Intervention of the Council on Cardiovascular Radiology and Intervention. Circulation. 2009 Feb 24;119(7):1056-65. Epub 2009 Feb 2.
Risks related to exposure to ionizing radiation The hypotheticalcomplication of diagnostic radiation exposurethat is of greatest concern, the risk of inducing malignancies,is a stochastic or random effect… Nothreshold below which radiation cannot cause malignanciesand that the risk of malignancies increases linearlywith radiation dose. Age- & genderaveragedlifetime risk of dying of a malignancy attributable toradiationexposure was estimated to be 5-7.9% of the general population per 1 Sv of E In individualsreceiving an estimated E <100 mSv, the relative risk ofdeveloping solid tumors was not statistically significantlydifferent from no increased risk Gerber TC, et al. Ionizing radiation in cardiac imaging: a science advisory from the American Heart Association Committee on Cardiac Imaging of the Council on Clinical Cardiology and Committee on Cardiovascular Imaging and Intervention of the Council on Cardiovascular Radiology and Intervention. Circulation. 2009 Feb 24;119(7):1056-65. Epub 2009 Feb 2. National Council on Radiation Protection and Measurements (NCRP).Risk Estimates for Radiation Protection. Bethesda, Md: National Councilon Radiation Protection and Measurements; 1993. Report No. 115.
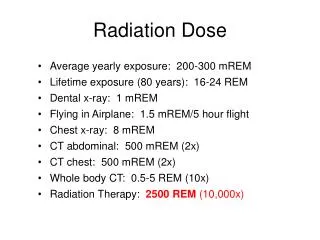
Risk associated with activities in daily life Allpeople are exposed to background radiation due to cosmicrays, radon, and other low-level radiation sources that onaverage amount to ≈3 mSv per year (range, 1 to 10 mSv) This makes it difficult todiscern between the risk attributable to a single exposure tomedical radiation and the risk of the exposure to naturalbackground radiation The population-averagedlifetime risk of developing a malignancy in the United Statesis 41%, and the risk of dying of a malignancy is 21% The estimated increase in the lifetime risk of dyingof a malignancy associated with 10 mSv (typical CCTA) of ionizing radiation is≈0.05% The relative risk of lung cancer ranged from 4.9 inindividuals who smoked 1 to 15 cigarettes per day to 13.3in individuals who smoked >25 cigarettes per day. The relative risk of lung cancer associated withan E of 1000 mSv (app. 50 to 100 CCTAs) was 2.2. United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR). Epidemiological studies of radiation and cancer. Paper presented at: 54th Session of UNSCEAR; May 29–June 2, 2006; Vienna, Austria. Ries LAG, et al. SEER Cancer Statistics Review, 1975–2004. Bethesda, Md: National Cancer Institute; based on November 2006 SEER data submission, posted to the SEER Web site, 2007. Tables I-14 and I-17: Lifetime risk (percent) of being diagnosed with cancer and lifetime risk (percent) of dying from cancer, by site and race/ethnicity. Available at http://seer.cancer.gov/csr/1975_2005/results_merged/topic_lifetime_risk.pdf. Accessed January 1, 2009. Pierce DA, et al. Joint effects of radiation and smoking on lung cancer risk among atomic bomb survivors. Radiat Res. 2003; 159:511–520.
Recommendations by AHA Science Advisory Committee onCardiac Imaging Imaging studies that expose patients to ionizingradiation should be ordered only after thoughtful considerationof the potential benefit to the patient and inkeeping with established appropriateness criteria Considerations should includeoptions for answering the clinical question at hand bymeans that do not use ionizing radiation or choosing thetype of study that exposes the patient to the lowest amountof radiation. Routine surveillance radionuclide stress tests or CCTA in asymptomatic patients at low risk for ischemic heartdisease are not recommended because there are no prospective,randomized trials that demonstrate that CCTA can convey survival benefit Once it has been established that CCTA is needed, every effort shouldbe made to reduce patient dose while balancing imagenoise and quality sufficient for confidentinterpretation Gerber TC, et al. Ionizing radiation in cardiac imaging: a science advisory from the American Heart Association Committee on Cardiac Imaging of the Council on Clinical Cardiology and Committee on Cardiovascular Imaging and Intervention of the Council on Cardiovascular Radiology and Intervention. Circulation. 2009 Feb 24;119(7):1056-65. Epub 2009 Feb 2.
CCTA, Images, example Contact: Ladislav.Pavic@sunce.hr