Download

1 / 167
1.67k likes | 2.32k Views
TARRSON FAMILY ENDOWED CHAIR IN PERIODONTICS. UCLA SCHOOL OF DENTISTRY. SECTION OF PERIODONTICS. Presents. Dr. E. Barrie Kenney Professor & Chairman Section of Periodontics. Dr. Heddie O. Sedano Professor Emeritus & Lecturer Section of Periodontics. PHASE ONE THERAPY. (INITIAL THERAPY).

E N D
UCLA SCHOOL OF DENTISTRY SECTION OF PERIODONTICS
Presents Dr. E. Barrie KenneyProfessor & ChairmanSection of Periodontics Dr. Heddie O. Sedano Professor Emeritus & Lecturer Section of Periodontics
PHASE ONE THERAPY (INITIAL THERAPY)
Comprehensive • Emergency Therapy • Examination Diagnosis and Treatment Plan • Phase one therapy (initial therapy) • Evaluation of phase one therapy • Phase two therapy • Evaluation of phase two therapy • Maintenance therapy
Phase two therapy • Periodontal surgery • Dental implants • Crown and bridge • Removable partial dentures
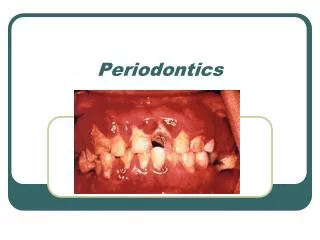
NECROTIZING ULCERATIVE GINGIVITIS (NUG) EMERGENCY THERAPY
Two weeks NUG resolved by root planning and good oral hygiene Proceed to complete examination and diagnosis
Phase one therapy • Control of plaque • Control of diet • Control of systemic factors • Control of oral malodor and taste abnormalities • Control of tobacco smoking
Presence of plaque in red for 4 surfaces of each tooth CONTROL of PLAQUE
Need to stress floss or interdental brush utilization Presence of interproximal plaque is prominent
Plaque and bleeding scores at 4 time periods Progressive improvement to less than 20% of surfaces with plaque
CORRELATION OF MANUAL DEXTERITY AND KNOWLEDGE WITH ORAL HYGIENE
CORRELATION COEFFICIENTS BETWEEN RIGHT HAND DEXTERITY AND BUCCO-LINGUAL PLAQUE IN 59 ADULTS DAY 0 0.41 DAY 7 0.38 DAY 14 0.33
CORRELATION COEFFICIENTS BETWEEN KNOWLEDGE AND BUCCO-LINGUAL PLAQUE DAY 0 0.38 DAY 7 0.32 DAY 14 0.30
Three weeks following compliance with excellent oral hygiene and plaque control
Brush is vibrated by bass technique of oral hygiene Soft brush positioned at 45° to gingiva
Best used for interproximal plaque when interdental papillae are present Dental Floss
Interdental brush Tuft brush
Best used when interdental papillae are reduced Interdental brush
Rubber interdental stimulator Least efficient interproximal cleaner
Use of gauze to clean distal surface of teeth adjacent to edentulous areas Gauze is most efficient for these teeth
Electric brushes used for patients with poor manual dexterity Electric brushes can motivate some patients to improve their oral hygiene
Clinical Evaluation of the Efficiency and Safety of aNew Sonic Toothbrush Johnson, B.D., McInnes, C., J. Periodontol 65:692, 1994
51 subjects got either Sonicare orhand brush. Instructed in use orModified Bass Technique withOral B 30.
Plaque scores, gingivitis scoresand sulcular bleeding scores at0, 1, 2, 4 weeks. 29 subjects seen at 6 months
All subjects got timer and did notuse floss mouth rinses or otheroral hygiene aids for first 4 weeks.
No increase in gingival recessionor other oral lesions associatedwith either brush at 6 months.
Comparison of an Oscillating Rotating Electric Toothbrush and a Sonic Toothbrush in Plaque Removing Ability Van Der Weijden, S.A., Timmerman, M.F., Van Der Velden, V. J Clin. Periodontol 23:407, 1996
35 non dental students given aSonicare and a Braun Oral B plakcontrol brush and instructed to useeach brush every other day.
2 weeks later subjects no brushingfor 24 hours then reevaluated thenmouth brushed by an examinersplit mouth using both brushes.
They repeated this 4 weeks laterwith brushing using Zendiumtoothpaste by the students.
At end of study they could keepone brush. 34 out of 35 keptBraun brush.
Clinical efficacy of flossing versus use of antimicrobial rinses.Zimmer. S, et al J. Periodontol. 2006 77:1380
156 patients used brush +daily rinse 0.06% chlorhexidine 0.025% fluoride or brush+ 0.1% cetylpyridiniumchloride +fluoride or brush + floss or brush alone.Evaluated at 8 weeks.
CHX NaF 1.58 CPC/NaF 1.54 FLOSS 2.10 BRUSH 2.00 / MODIFIED PROXIMAL PLAQUE INDEX
Papilla Bleeding Index CHX /NaF 0.67 CPC/NaF 0.75 FLOSS 0.77 BRUSH 0.89
Additional effect of dentifrices on the instant efficacy of tooth brushing.Paraskevas S .et al J. Periodontol.2006 77:1522
3 toothpastes used in 40 patients each after 48 hours plaque accumulation.Split mouth hand brush with or without paste.
Tooth paste gave average of 3% more plaque than brush alone.More abrasive pastes no more effective.
CONTROL OF DIET More benefit comes from reduction of sucrose in diet so less caries and less plaque minimal effect on gingival inflammation from other dietary modifications
CONTROL OF SYSTEMIC FACTORSCONSULT WITH PATIENT’S M.D. Control of Hemostasis Control of Bacteremia Control of Diabetes Control of Medications
CONTROL OF ORAL MALODORAND TASTE ABNORMALITIES Plaque control is most predictable way to reduce oral malodor together with daily tongue scarping to reduce bacterial load of oral cavity.