Download
1 / 20
220 likes | 527 Views
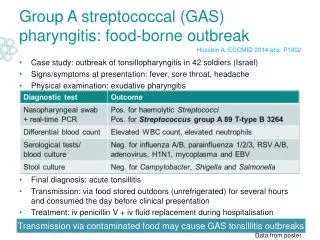
Neonatal Group B Streptococcal Infections. Perinatal CDC Prevention Guidelines Priscilla Joe, MD. The Disease. Leading cause of early-onset sepsis in US Prior to intrapartum prophylaxis: 8,000 cases/year or 2/1000 live births Reduced now to 1,600 cases/year or 0.6/1000 live births

E N D
Neonatal Group B Streptococcal Infections Perinatal CDC Prevention Guidelines Priscilla Joe, MD
The Disease • Leading cause of early-onset sepsis in US • Prior to intrapartum prophylaxis: 8,000 cases/year or 2/1000 live births • Reduced now to 1,600 cases/year or 0.6/1000 live births • Perinatal GBS disease burden • Neonatal illness/death, long-term disability • Maternal morbidity
Mother to Infant Transmission GBS colonized mother 50% 50% Non-colonized newborn Colonized newborn 98% 2% Early-onset sepsis, pneumonia, meningitis Asymptomatic
Colonization Rates • GBS Carriers • 10% - 30% of women • Higher in African Americans and nonsmokers • Clinical signs not predictive • Dynamic condition • Risk factor for early-onset disease: GBS colonization at delivery • Prenatal cultures late in pregnancy predict delivery status
Additional Risk Factors forEarly-Onset GBS Disease • Obstetric: prolonged rupture of membranes, preterm delivery, intrapartum fever • GBS bacteriuria • Previous infant with GBS disease • Demographic (African American, young age) • Immunologic (low antibody to GBS capsular polysaccharide)
Prevention of Perinatal GBS Disease • Intrapartum antibiotics • Highly effective at preventing early-onset disease in women at risk for transmission of GBS to their newborns • Challenge: How best to identify women at risk?
Rates of Early-Onset GBS Disease by Prenatal Colonization & Risk Factors Col: prenatal vag/rect culture RF: risk factors (gest. <37 wks, ROM >18 hr, fever > 37.5°C) Boyer & Gotoff, Antibiot Chemother 1985.
First U.S. Consensus Recommendations(CDC '96, ACOG '96, AAP '97) • Screening-based approach: • 35-37 wks culture, offer intrapartum antibiotic prophylaxis (IAP) to GBS carriers and to preterm unless neg. culture result available, or • Risk-based approach: • IAP to preterm, membrane rupture>18 hours, or intrapartum fever (T>38°C) Both strategies also give IAP to women with GBS bacteriuria, or previous infant with GBS disease
Why is screening more protective than the risk-based approach? • Broader coverage of at-risk population • Captures colonized women without obstetric risk factors (18% of all deliveries) • Antibiotic effectiveness in this cohort, based on birth survey data: 89% (64-97%) Schrag et al, NEJM 2002, 347:233-9
Intrapartum Prophylaxis: Indications • Previous infant with invasive GBS disease • GBS bacteriuria during current pregnancy • Positive GBS screening culture during current pregnancy (unless a planned c-section, in the absence of labor or amniotic membrane rupture) • Unknown GBS status AND any of the following: • Delivery at < 37 weeks’ gestation • Amniotic membrane rupture >18 hours • Intrapartum temperature >38.0°C
Intrapartum Prophylaxis NOT Indicated • Prior pregnancy with a positive GBS screening culture (unless culture positive ALSO during current pregnancy) • Planned c-section performed in the absence of labor or membrane rupture (regardless of maternal GBS culture status) • Negative vaginal and rectal GBS screening culture during the current pregnancy, regardless of intrapartum risk factors
Early Onset Disease • Presentation within 1st 24 hrs, 0 - 6days • 75% of cases of GBS disease • Vertical transmission • Sepsis 25-40% • Pneumonia 35-55% • Meningitis 5-10% • Mortality 5%; higher in preterm infants • Due to opsonin deficiency, limited maternal antibody transfer, limited maternal capsular antibody
Late Onset Disease • 3-4 weeks after birth, range 7d-3mo • Term and preterm infants equally susceptible • Serotype III most common and predominant cause of meningitis • Bacteremia and meningitis • Osteomyelitis, septic arthritis, and cellulitis • Horizontal transmission (hospital, community, mother) • Incidence unchanged with intrapartum prophylaxis
Treatment of Asymptomatic Neonates • 24-48 hr observation period for infants with pretreated mothers • Routine use of antibiotics in infants whose mothers received adequate treatment is not indicated
Diagnosis • Blood, CSF, ETT cxs • CBC • CRP • CXR
Treatment of GBS Disease • Ampicillin and Gentamicin • 7-10 days for uncomplicated bacteremia • 14 days for uncomplicated meningitis • 21-28 days for meningitis complicated by abscesses, ventriculitis • 4-6 weeks for osteomyelitis or endocarditis
References • http://www.cdc.gov/groupbstrep/gbs/hospitals_guidelines.Neonatal.htm