Download

1 / 47
510 likes | 926 Views
Swallowing Pills. G. Carnaby & M. Crary Swallowing Research Laboratory. Swallowing. Swallowing is something that we do 2,000 to 3,000 times every day, yet it is a very complex act requiring many muscles coordinated by the brain and brainstem.

E N D
Swallowing Pills G. Carnaby & M. Crary Swallowing Research Laboratory
Swallowing • Swallowing is something that we do 2,000 to 3,000 times every day, yet it is a very complex act requiring many muscles coordinated by the brain and brainstem. • The swallow mechanism is innervated by 7 pairs of nerves and 26 muscle groups
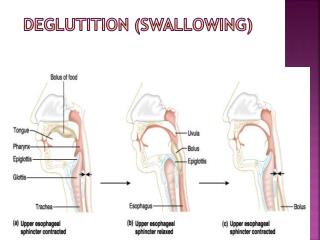
Normal Swallowing • Three phases of swallowing • Oral phase • Pharyngeal phase • Esophageal phase
Phases of swallowing • Oral phase. Biting and chewing takes place in the mouth. During this stage, food is broken down into smaller pieces and mixes with saliva. This preparation stage is where the pleasure of eating is derived.
Oral phase • In this voluntary stage, the tongue pushes the food or liquid to the back of the mouth, where it is positioned to pass into the throat (pharynx). When this stage is completed, there should be no food or liquid remaining in the mouth.
Pharyngeal phase • During this phase, the palate, the soft structure that hangs in the back of the throat, elevates to prevent food or liquid from entering the nose. The voice box closes to prevent food from entering the windpipe, and a muscle at the low end of the pharynx relaxes to allow food to enter the esophagus.
Fluoroscopic Lateral View – OroPharyngeal Components • Video 1 – slow motion oropharyngeal swallow
Swallow Variants - Accommodation • Video 2 – Bolus Accommodation examples
Endoscopic View - Oropharyngeal • Video 3 – endoscopic view normal oropharyngeal swallow
Esophageal phase • A series of coordinated muscle contractions pushes the food down the esophagus (food tube) and into the stomach.
Esophageal Clearance - Fluoroscopy • Video 4 – example of fluoroscopic clearance
University of Florida Swallowing Research Laboratory http://srl.phhp.ufl.edu
Swallowing Research Laboratory • Research Foci • Study of normal and abnormal swallowing physiology • Development of innovative assessment and treatment ‘tool’s for adult dysphagia • Current Projects (examples) • Prevention of dysphagia in head/cancer • Swallow frequency to screen for dysphagia in stroke • Reflux and swallow frequency in acute stroke • Oral morbidities in head/neck cancer • Swallow abilities in community dwelling elderly
Swallowing Research Laboratory • Measurement Capabilities • Videofluoroscopy • Transnasal endoscopy • Transnasalesophagoscopy • Lingual-palatal pressure measurement • Pharyngeal and upper sphincter manometry • High Resolution Manometry • MRI • sEMG • Respiratory measures • And More!
Difficulty swallowing • “Dysphagia (dis-fag-ia) • Defined as difficulty swallowing or the inability to swallow food or fluids”
Epidemiology of dysphagia • Estimated to affect 22% of the world’s population >50 years of age • Swallowing disorders are becoming a major source of disability –estimated 17 million adults in the US alone • Up to 30% of patients in hospitals • ~60% of residents in nursing homes • Probably 14% of people >65 years of age living in the community • Approximately 10 million children in the US
Disorders of swallowing • Can occur in all age groups • May be a result of many different medical conditions • Can be an acute problem or progress slowly over a long period of time • Early identification and involvement of health professionals offers a good prognosis for swallowing disorders. • Abnormalities of swallowing could be secondary to defects in any of the stages of swallowing enumerated above.
Many people with dysphagia can go unrecognized or undiagnosed until a major medical event occurs.
Additional Definitions • Aspiration: Passive entry of any food item into the trachea (eg, during inhalation), although the term often is used to denote any entry of material into the trachea in any manner • Penetration: Active entry of any food item into the trachea (eg, during swallowing), although the term often is used to denote the entry of any material into the laryngeal vestibule
Diagnostic tools • Videofluoroscopicprocedure (xray video) • Most widely used determine physiology of swallow • Other evaluation tools • Fiberoptic endoscopic examination • Ultrasound • Electromyography • Manometry
Videofluoroscopy • Videofluoroscopic procedure • Also known as modified barium swallow • A radiographic study of a person’s swallowing mechanism that is recorded on videotape
Videos - dysphagia • Video 5 - Zenker’s Diverticulum
Dysphagia • Video 6 – Cricopharyngeal Bar
Dysphagia • Video 7 – Stricture in PES with NPR
Pills and More • Video 8 – Liquids pass but not the tablet!
Pills and More • Video 9 – Pills stick in throat and chest
Endoscopy - dysphagia • Video 10 – Endoscopic View Dysphagia in Elderly
Swallowing PillsEpidemiology Online National US survey 2003 [ n=679, 513 – 18-64yrs; 166 ≥65yrs] • 40%- Report difficulty with swallowing pills • 51% women /27% men • 18-64 (44%); ≥65yrs (26%)
Impact of difficulty taking pills • 14% delayed dosage • 8% skipped a dose • 4% discontinued • 14% discussed issue with a health care provided • failure to follow dosing recommendations is associated with poorer health outcomes
Impact of difficulty taking pills • 1/5 hesitate before taking pills • Shape (84%) • Size (29%) • 1/10- choose based upon anticipated difficulty to swallow • Women (14%) • Men (4%)
Pill swallowing – Physiologic effects • Little data on the alterations in the swallow system that occurs with pills • Swallowing a learnt complex motor task… • Shibamoto et al (2007) • fMRI to view cortical brain activation with pill swallowing (11mm X 2mm columnar capsule) n=21 healthy persons • different brain areas activated during capsule swallowing- i.e. cerebellum
swallow Tongue movement Finger tapping
Food Sticking in Throat Study • Review of outpatient with complaints of food/liquid sticking in throat • Evaluation of fluoroscopic videos to identify • Any confirmation that something does stick • Where it sticks • Cause of ‘sticking’ • What material best identifies the problem
Methods • 315 outpatients were reviewed • 117 patients c/o solid “sticking” • 24 patients c/o solid and liquid “sticking” • Total of 141 patients with the complaint • Prevalence = 45%
Results • Mean Age (in years) : 61.46 • Female:Male = 88:53 • Positive fluoroscopic findings • 108 patients = 77%
Anatomic vs. Physiologic findings • 15% of the positive cases = anatomic • strictures, pouches etc. • 85% of the positive cases = physiologic • esophageal dysmotility, achalasia etc.
15% of positive cases had anatomic obstructions UES = Upper Esophageal Spincter 15% of positive cases
85% of positive cases had physiologic obstructions UES = Upper Esophageal Sphincter LES = Lower Esophageal Sphincter 15% of positive cases
Conclusions • 45% Prevalence of food sticking symptoms • 27% correctly localized obstruction in “throat” • Anatomic obstructions, primarily in UES • Better localization for anatomic obstructions • 73% incorrectly localized obstruction upward in throat • Primarily physiologic obstructions
Summary • Swallowing is a complex process with interplay among major anatomical components • Oral • Pharyngeal • Laryngeal • Dysphagia may be overt or covert • Many patients with covert of mild dysphagia remain total oral feeders and take meds orally • Food sticking is a common complaint in overt/covert • Pills sticking is a common complaint • Pill swallowing is different from food/liquid • Physiology is different • Neurology is different