Download
1 / 68
700 likes | 1.08k Views
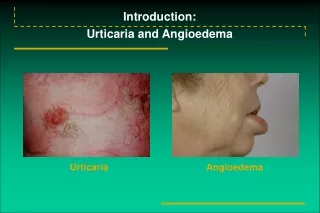
Urticaria 11/12/2010. BY: MOHAMMED ALSAIDAN. Urticaria . Recurrent wheals that are usually pruritic , pink-to-red edematous plaques that often have pale centers May occur anywhere on the skin, Any age Itch is relieved more by rubbing rather than by scratching

E N D
Urticaria11/12/2010 BY: MOHAMMED ALSAIDAN
Urticaria • Recurrent wheals that are usually pruritic, pink-to-red edematous plaques that often have pale centers • May occur anywhere on the skin, Any age • Itch is relieved more by rubbing rather than by scratching • Purpura rather than excoriations
Urticaria • lifetime occurrence of urticaria in the general population ranges from 1% to 5%. • Classification: clinical characteristics Vs. etiology
pathogenesis • The mast cell is the principal effector cell of urticaria • All mast cells express high-affinity IgE receptors (FceRIs) that enable the involvement in IgE-dependent allergic reactions, leading to degranulation • Mast cell degranulation also occurs through a variety of other mechanisms • These stimuli initiate calcium and energy-dependent steps
pathogenesis • One study has shown that the serologic immune profile of patients with chronic autoimmune urticaria is a mixed T helper-1 (Thl)/ Th2 pattern with a slight Th2 predominance
pathogenesis • Histology of chronic urticaria (both idiopathic and autoimmune) demonstrates a perivascular non-necrotizing infiltrate of lymphocytes consisting of a mixture of Thl and Th2 subtypes, plus monocytes, neutrophils, eosinophils, and basophils.
Chronic urticaria aetiology • Most cases of chronic urticaria remain idiopathic • 35-50% of chronic urticaria cases are related to autoimmunity, specifically the presence of autoantibodies to (FceRl) located on mast cells, 5-10% have IgG antibodies to IgE itself. • Other identifiable causes of chronic urticaria include: IgE-dependent, complement-mediated, or immune complex deposition. • Non-immunologic causes ?
Genetics • Prevalence of the disease was much higher among first-degree relatives than in the general population. • Patients with chronic idiopathic urticaria have an increased frequency of HLA-DR4 and HLA-D8Q. • HLA-DR4 is strongly associated with autoimmune chronic urticaria.
Food • Food allergy and food additives such as preservatives and coloring agents do not appear to be significant causes of chronic urticaria • Most physicians feel that elimination diet approach is unnecessary • Food allergies typically would cause a reaction within 30 minutes of ingestion
Autoimmune associations • Autoimmune conditions associated with chronic urticaria : • Thyroid diseases • vitiligo • insulin-dependent diabetes mellitus • rheumatoid arthritis • pernicious anemia
Thyroid diseases • Both Hashimoto thyroiditis and Graves disease have been associated with chronic urticaria. • Antithyroid antibodies, antimicrosomal antibodies, or both have been found in up to 27% of patients with chronic urticaria • Positive ASST result had significantly more autoimmune thyroid disease • No evidence that the antibodies involved in thyroid disorders play a role in the pathogenesis of chronic urticaria
H.pylori • Increased frequency of H. pylori IgG antibodies in patients with chronic urticaria • Helicobacter pylori, has an immunogenic cell envelope, can reduce immune tolerance and induce autoantibody formation, such as anti-FceRI. • Efficacy of eradication of H. pylori in the treatment of chronic urticaria is a controversial (Federman et al., 2003) • Association with (MALT) lymphoma and gastric adenocarcinoma?
Malignancy + other diseases • There is no association between chronic urticaria and malignancy • Little supporting evidence for association between urticaria and occult infections such as: • dental abscesses • gastrointestinal candidiasis • Parasitic infections such as intestinal in endemic areas. • The fish nematode Anisakis simplex (IgG4 antibodies). • hepatitis C (conflicting results) • No conclusive evidence is available linking chronic urticaria with hepatitis B, EBV, CMV, or HIV.
Acute Urticaria • Wheals for <6 weeks • Individual lesions typically resolve in <24 hours • More commonly in pediatric population • Associated with atopy. • 20% progress to chronic or episodic
Acute Urticaria • IgE dependent : • foods, drugs, insects, contact, or parasites • Direct mast cell degranulation and proinflammatory mediator: • Opioids, muscle relaxants, radio-contrast agents, and vancomycin. • Complement-mediated acute urticaria : • serum sickness, transfusion reactions, and viral or bacterial infections • Metabolism of arachidonic acid: • aspirin and NSAIDs
Chronic Urticaria • Cutaneous wheals on a regular basis (usually daily) for >6 weeks with individual lesions lasting from 4 to(2436) hours. • Establishing cause and effect is difficult and many cases remain idiopathic. • Significant portion of idiopathic urticarias may have an autoimmune etiology • Chronic urticaria is more prevalent in female patients, occurring at a 2 : 1 female-to-male ratio
Contact Urticaria • Urticarial wheals at the site where an external agent makes contact with skin or mucosa. • Allergic (IgE-mediated)contact urticaria occurs in persons sensitized to environment allergens such as grass, animals, or latex gloves • Non-allergic contact urticaria occurs as a result of the direct effects of urticants on blood vessels. E.g. sorbic acid in eye solutions, cinnamicaldehyde in cosmetics, and chemicals from the stinging nettle
Physical Urticaria • Typically localized to the stimulated area and resolve within 2 hours with the exception of delayed (pressure and dermatographism) • Symptomatic dermatographism - the most common form of physical urticaria - is not associated with systemic disease, atopy, food allergy, or autoimmunity.
Physical Urticaria Delayed-pressure urticaria: • May present with systemic symptoms (malaise, influenza-like symptoms, and arthralgias) • Deep erythematous swellings at sites of sustained pressure to the skin after a delay of 30 minutes to as long as 12 hours. • Waistline ,elastic band of socks. • Many patients with delayed-pressure urticaria also have concurrent chronic idiopathic urticaria.
Physical Urticaria Cholinergic urticaria • The second most common type of physical urticaria • Around 3mm wheal surrounded by an obvious flare in response to physical exertion, hot baths, or sudden emotional stress, Adrenergic urticaria • blanched, vasoconstricted skin surrounding small pink wheals.
Schnitzler syndrome • Chronic urticaria vs. Urticarialvasculitis! • Recurrent non-pruriticwheals • Intermittent fever, bone pain, arthralgias or arthritis, an elevated (ESR), and a monoclonal IgMgammopathy. • +/- IgG antibodies directed against (IL)-l • Biopsies of lesions often demonstrate an increased polymorphonucleocyte count with occasional leukocytoclasia.
Schnitzler syndrome • 10% to 15% of patients subsequently develop a lymphplasmic malignancy, such as Waldenstrommacroglobulinemia, lymphoplasmacytic lymphoma, or IgM myeloma • Anakinra, an IL-1 receptor antagonist, appears to be a promising agent • Rituximam and thalidomide have also been used
Muckle-Wells syndrome • An autoinflammatory disorder associated with cold-induced autoinflammatory syndrome-1 gene mutations • Characterized by urticaria, arthralgias, progressive sensorineural deafness, and amyloidosis
(PUPPP) • Also known as polymorphic eruption of pregnancy • The most common dermatosis associated with pregnancy. Its lesions are often urticarial and involve the trunk, particularly abdominal striae. • Benign, self-resolving course with an onset in the third trimester. • Serious DDx : pemphigoidgestationis, a bullouspemphigoid like-disorder associated with pregnancy
Urticarialvasculitis • Rare, with reported ranges of 1-10% in patients with chronic urticaria • In contrast to chronic urticaria, tend to last longer than 24 h. • Associated with burning and pain in addition to itching • Healing with purpura or petechiae
Urticarialvasculitis • Skin biopsy typically shows evidence of leukocytoclasticvasculitis. • Typically a component of a chronic systemic illness such as: • systemic lupus erythematosus • hypocomplementemicurticarialvasculitis syndrome • Sjogren syndrome • mixed cryoglobulinemia.
Diagnostic work up • A detailed history is usually adequate to establish a diagnosis of chronic urticaria • if laboratory tests are warranted, ESR and WBC count with differential • Test for H. pylori infection, If no cause found • Thyroid function tests and tests for thyroid antibodies are necessary only when symptomatic • Skin Bx for suspected urticarialvasculitis
Diagnostic work up • Challenge testing is indicated when a patient is being evaluated for a physical urticaria • Patients with angioedema but without urticaria should have C4 levels measured to screen for CI-inhibitor deficiency • CI-inhibitor levels can be measured if the C4 level is low
Chronic autoimmune urticaria • Patients with autoantibodies have: • more wheals with a wider distribution • higher itch scores • more systemic symptoms • and lower serum IgE levels • more likely to require and benefit from immunosuppressive therapy • Results with ELISA and immunobinding techniques have been disappointing • A decrease in basophils (basopenia) • ASST is currently not widely used (chronic autoimmune urticaria, more aggressive and resistant than chronic idiopathic urticaria)
ASST • patient's own serum (during a flare) is injected intradermally into uninvolved skin of the forearm • Saline and histamine controls are injected at the same time. • the serum-injected site is 1.5 mm> saline-injected site • The sensitivity (65-81%) and the specificity (71-78%)