Download
1 / 37
530 likes | 1.97k Views
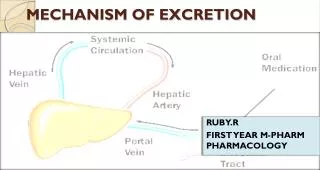
MECHANISM OF EXCRETION. RUBY.R FIRST YEAR M-PHARM PHARMACOLOGY. EXCRETION. Excretion is the passage out of systematically absorbed drug. Drugs are eliminated from the body either unchanged by the process of excretion or converted to Metabolites. Polar compounds more efficiently eliminated.

E N D
MECHANISM OF EXCRETION RUBY.R FIRST YEAR M-PHARM PHARMACOLOGY
EXCRETION • Excretion is the passage out of systematically absorbed drug. Drugs are eliminated from the body either unchanged by the process of excretion or converted to Metabolites. • Polar compounds more efficiently eliminated.
IMPORTANCE OF EXCRETION • Determining the duration of drug action. • Determining the rate of drug elimination.
ROUTES OF EXCRETION RENAL EXCRETION NON RENAL EXCRETION Biliary excretion. Pulmonary excretion. Salivary excretion. Mammary excretion. Skin / Dermal excretion. Gastrointestinal excretion. Genital excretion.
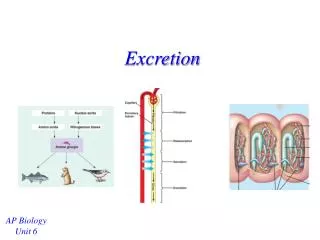
URINE (RENAL EXCRETION) • The kidney is responsible for excreting all water soluble substances. • The three principalprocesses that determine the urinary excretion of a drug are • Glomerular filtration • Tubular secretion and • Tubular reabsorption(mostly passive back-diffusion)
Net renal excretion = (G.F + tubular secretion)-tubular reabsorption
1.1 Glomerular filtration • Molecular weight below about 20000 to diffuse into the glomerular filtrate. • Nonprotien bounded drug with the exception of macromolecules such as heparin cross the barrier freely. • Glomerular filtration of drug depend on Plasma protein binding Renal blood flow
1.2. TUBULAR REABSORPTION • This occurs by passive diffusion and depend on Lipid solubility Ionization of drug at the existing urinary PH • Lipid-soluble drugs are therefore excreted poorly, whereas polar drugs of low tubular permeability remain in the lumen.(digoxin, quaternary ammonium compounds and aminoglycoside antibiotics parallels g.f.r. ) • Weak bases ionize more and are less reabsorbed in acidic urine vice versa • This is utilized for facilitating elimination of drug in poisoning Urine is alkalinized in barbiturate and salicylate poisoning Elimination of weak bases (morphine and amphetamine) Can be enhanced by acidifying urine( "ion trapping.“)
TUBULAR SECRETION (ACTIVE PROCESS) • Active transfer of organic acids and bases by two separate classes of relatively nonspecific transporters (OAT and OCT) which operate in the proximal tubules. In addition, efflux transporters p-gp and MRP2 are located in the luminal membrane of proximal tubular cells • Protein bounded drugs are eliminated
Factors influencing renal drug excretion Gender:Renal excretion is 10% lower in female than in males. Age : Renal function⇓ 50% with age (25 –75 yr)Pregnancy: Renal function⇑ 50%Disease: Renal disease, heart failure
Alteration of renal excretion of drugs 1. Competitive inhibition of tubular secretion (i) Salicylates block uricosuric action of probenecid and sulfinpyrazone and decrease tubular secretion of methotrexate. (ii) Probenecid decreases the concentration of nitrofurantoin in urine, increases the duration of action of penicillin/ampicillin and impairs secretion of methotrexate. (iii) Sulfinpyrazone inhibits excretion of tolbutamide. (iv) Quinidine decreases renal and biliary clearance of digoxin by inhibiting efflux carrier P-gp.
2. Influence of pH • Sodium bicarbonate used to alkalinize urine; ie⇑ pH,⇑ ionization of weak acid (salicylate, methotrexate),⇓ tubular reabsorption →⇑ excretion. •Ammonium chloride used to acidify urine to ⇑ excretion of basic drugs (amphetamines).
3. Influence of urinary flow rate •⇑ urinary flow rate dilutes drug conc. in tubule →⇓ conc. gradient for passive reabsorption of drug →⇑ excretion. • Urine flow increases in meprobamate poisoning •⇓ urinary flow rate has the opposite effect
2. Biliary and Fecal Excretion • Drugs present in faeces is derived from bile. Liver cells actively secrete various substances, including drugs, from plasma to bile by means of transport systems. • Organic acid by OATP • Organic base by OCT(Organic cation transport) • Lipophilic - P-gp and BCRP (breast cancer resistance protein) • Conjugated metabolites of drugs - MRP2 e.g., glutathione conjugates, glucuronides, and some sulfates
3.exhaled air • Volatile substance and gases • Mechanism-simple diffusion passive diffusion from the blood into the alveolus, following a concentration gradient. • The rate of loss of gases is not constant; it Depends on the rate of respiration Pulmonary blood flow. The degree of solubility of a gas in blood • Nitrous oxide, which are not very soluble in blood, will be excreted rapidly Ex: General Anaesthetics, Paraldehyde, Alcohol.
4.SALIVA • The pH of saliva varies from 5.8 to 8.4 • Excretion mainly depends on the diffusion of the un-ionized lipid-soluble form of the drug across the epithelial cells of the glands. • Salivary recycling-- drug excreted in saliva is probably swallowed • Ex: Iodine, Metronidazole, Lithium, Phenytoin,Caffeine, Theophylline. Example of drug excreted through tears: Rifampin
5. SWEAT (SKIN) • Diffusion of the non-ionized lipid-soluble form of drugs through the epithelial cells of the glands and depends on the pH. • Passive excretion of drugs and their metabolites through skin is responsible to some extent for urticaria and dermatitis and other hyper sensitive reactions.
Drugs excreted through hair • They may be deposited from the capillaries, which supply blood to the follicles, or they may be excreted in the sebum, oil, or sweats that coat the hair shafts. • Arsenic is getting accumulated on hair follicle after prolonged use .it is used to detect arsenic poisoning
6.MILK • Ph of milk varies from 6.4 to 7.6 • Mechanism of elimination is passive diffusion • Basic compounds may be slightly concentrated in milk • Non-electrolytes, such as ethanol and urea, readily enter breast milk and reach the same concentration as in plasma, independent of the pH of the milk.
ADVERSE EFFECTSDiscoloration of teeth with tetracycline and jaundice due to interaction of bilirubin with sulfonamides. Nicotine is secreted in the milk of mothers who smoke.
7. INTESTINE • Laxatives like senna and cascara, which mainly act on bowel, are partly excreted into that area from the blood stream, after their absorption from small intestine. • Heavy metals in particular zinc. also excreted through intestine and can produce intestinal ulceration.
DRUG CONCENTRATIONS IN SEMEN • Mechanism is assumed that the boundary between the systemic circulation and the seminal compartment behaves as a lipid barrier, most drugs will enter by passive diffusion. • Ex: Antiretroviral-Druglike zidovudine and lamivudine
CLEARANCE (CL) • The clearance of a drug is the theoretical volume of plasma from which the drugis completely removed in unit time. I t can be calculated as • Where C is the plasma concentration.
Elimination of drug from the body may involve processes occurring in the kidney, the lung, the liver, and other organs. • Dividing the rate of elimination at each organ by the concentration of drug presented to it yields the respective clearance at that organ. Added together, these separate clearances equal total systemic clearance: • ClT = ClR+ClN.R Cl T = Total Clearance ClR = Renal Clearance ClN.R =NonrenalClearance
REFERENCES • Rang & dale's pharmacology 7th edition, BY H.Rang,M.M. Dale page no:34-36 • The pharmacological basis of therapeutics By Goodman & Gilman ,12th edition ,page no: 23-27 • Color Atlas of Pharmacology, 3rdEdn By Heinz lullman,Klausmohr. page no:36-39 • Basic & clinical pharmacology - 10th Ed. (2007) By Vishal. page no:57-59 • CLinical pharmacology Dr. P. Oh,AmanHussain, Leora Horn, page no:12-16 • Applied Biopharmaceutics & Pharmacokinetics, 5th EditionLeon Shargel, Susanna Wu-Pong, Andrew B.C. Yu, page no:23-26 • Introduction to pharacology 2nd edition ByanntredA,Holinger,page no:61-68 • Essentials of medical pharacology By K.D Thripathi, page no:34-37
Perform your original search, excretion of drug through skin, in Clinical ChemistrySearchClinical Chemistry 54: 172-180, 2008. First published November 2, 2007; 10.1373/clinchem.2007.092304 • Vree TB, Muskens AT, van Rossum JM. Excretion of amphetamines in human sweat. Arch IntPharmacodynTher 1972;199:311-317.[Web of Science] • MIECKOWSKI, T. Hair analysis as a drug detector. (NCJ156434). http://www.ncjrs.org/drgstest.htm • Google images of excretion