Download
1 / 30
320 likes | 884 Views
MALIGNANT DISORDER OF THE CERVİX. Assoc. Prof. Gazi YILDIRIM, M.D. Yeditepe University, Medical Faculty Dept of Ob&Gyn. Abnormal Cytologic Findings: (The TBS, 2001). AS cells : ASC – US (Atypical Squamous Cell Undetermined Significance)

E N D
MALIGNANT DISORDER OF THE CERVİX Assoc. Prof. Gazi YILDIRIM, M.D. Yeditepe University, Medical Faculty Dept of Ob&Gyn
Abnormal Cytologic Findings: (The TBS, 2001) • AS cells: • ASC – US (Atypical Squamous Cell Undetermined Significance) • ASC – H (Atypical Squamous Cell cannot exclude High grade) • LSIL (Low grade Squamous Intraepitelial Lesion) • HSIL(High grade Squamous Intraepitelial Lesion) • AG cells(Atypical Glandular Cell) • AGC – NOS (Not Potherwise specified) • AGC – favorneoplasia • AIS(adenocarcinoma in situ) • InvasiveCancer
Patogenez HPV normal hücreler minimal hücresel değişiklik LGSIL(CIN I) HGSIL (CIN II-III) İnvasiv kanser
CIN’lerin Seyri CIN’lerin Seyri Östör AG, Int J Gynecol Pathol,1993
Cervical Carcinoma • Theaverageage at diagnosis is 51 years • Over95 % of thepatientswithearlycancer of thecervix can be cured
Cervical Cancer Lifetime risk 0.8% Risk of dying 0.3% 15% of female cancers 4-6% Developed 20-30% Developing Incidence Preinv 29-30/100 000 Invasive 6-9/100 000
ETIOLOGY and EPIDEMIOLOGY • Risk factors for cervical cancer are the same as CIN • HPV is central to the development of cervical neoplasia (99 % of all cervical carcinomas), • HPV 16 => Squamous cell carcinoma • HPV 18 => Adenocarcinoma • Other risk factors: • Immuno suppresion • Infection of HIV • History of other sexually transmitted disseases • High parity • Oral contraceptive use, • Tobacco use
HPV and Cervical Cancer: pathogenesis Infection with high-risk HPV types Integration of HPV into the human genome Expression of viral genes Synthesis and upregulation of viral oncogenes (E6,E7) Host cell immortalization and malign transformation
Viral oncogenes and its functions • E6 p53 degradation, increased telomerase activity • E7 functional inhibition of pRB
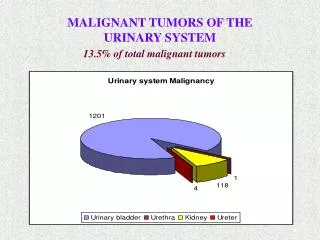
PATHOLOGY • Cervical Carcinomas • 70 – 75 % Squamous cell carcinoma • 20 – 25 % Adenocarcinoma • 3 – 5 % Adenosquamous carcinoma and undifferentiated carcinomas
CLINICAL STAGING • It is important to estimate the extent of the disease not only for prognostic purposes but also for treatment planning!!
Serviks Kanserinin Evrelemesi(FIGO2009) Evre I: Servikse sınırlı karsinom(corpus yayılımı gözardı edilir) Evre IA: yalnız mikroskobik olarak tanımlanır,gözle görülmez Evre IA1: İnvazyon derinliği ≤ 3mm, genişiği<7 mm Evre IA2: İnvazyon derinliği >3-5 mm,genişliği <7 mm Evre IB: servikse sınırlı klinik lezyon veya > evre1A preklinik lezyon Evre IB1: Lezyon ≤ 4 cm Evre IB2: Lezyon > 4 cm Evre II: Serviks dışına çıkmış,pelvik duvara ulaşmamış karsinom,2/3 üst vajen tutulumu var Evre IIA: Belirgin parametriyal tutulum yok IIA1: lezyon ≤ 4 cm IIA2:lezyon >4 cm Evre IIB: Belirgin parametriyal tutulum var Evre III: Pelvik duvara ulaşmış karsinom Evre IIIA: Pelvik duvara yayılım yok, 1/3 alt alt vajen tutulumu var Evre IIIB: Pelvik duvara yayılım var ve/veya hidronefroz veya nonfoksiyone böbrek Evre IV: Gerçek pelvis dışına ulaşmış karsinom Evre IVA: Komşu organlara yayılım(klinik veya biopsi ile kanıtlanmış olarak mesane ve rektum mukozası tutulumu var) Evre IVB: Uzak metastaz
Staging CLINICAL (FIGO, TNM) Chemical Studies X-Ray studies (IVP, etc) Endoscopic Examination Under General Anesthesia Lymphatic imaging interventions
27 40 57 122 510 Number of Patients with respect to stages IV IA III II IB
TREATMENT • Invasive carcinoma of the cervix spreads primarily by direct extension and lymphatic dissemination. • The therapy accomplished by either radical hysterectomy and pelvic lymphadenectomy, radiation with concominant chemotherapy or acombination thereof.
Surgery Radiation Chemoradiation therapy Combined Supportive Therapeutic Tools
Strategies in Treatment of Early Cervical Cancer Primary lesion Possible metastatic sites
TREATMENTof Early Stage Disease (Stage IA2 to IIA) • Radical hysterectomy and pelvic lymphadectomy • Radical Hysterectomy with pelvic lymphadenectomy is the surgical procedure for invasive cancer limited to the cervix (Stage I and II) • Stage IA1 => Type I Hysterectomy • Stage IA2 => Type II (Modified radical hysterectomy) • Stage IB-IIA => Type III Hysterectomy • Primary radiation with concominant chemotherapy
TREATMENTof Early Stage Disease (Stage IA2 to IIA) Indications • Positive lymph nodes • Positive or close resection margins • Microscopic parametrial involvement Adjuvant Post Operative Radiation
SPECIAL SITUATIONS • STAGE IA DISEASE • For a young woman desiring to maintain fertility, conization may be acceptable if: • Depth of invasion of 3 mm or less • Conization margins are negative • There is no evidence of lymphovascular space invasion • RADICAL TRACHELECTOMY
TREATMENTof Locally Advanced Disease (Stage IIB to IVA) • Primary radiation with concominant chemotherapy Stage 3b
TREATMENTof Disseminated Primary Disease (Stage IVB) • Chemotherapy
When the lymphatics are involved, tumor cells are carried to the regional pelvic lymph nodes.(parametrial, hypogastric, obturator, external iliac and sacral) • Ovarian involvement is rare, the liver and lungs are the most common sites of blood-borne metastasis rarely involves the brain, bones, bowels, adrenal glands, spleen or pancreas
Death can occur from • uremia, • pulmoner embolism or • hemorrhage from direct extension of tumor into blood vessel • Pyelonephritis, vesicovaginal and rectovaginal fistules are possible and may cause life-threatening sepsis
Prevention of Cervical Cancer Counselling Barrier contraceptives Monogamy Screening Vaccine Diet
PREVENTION • Risk factors must be recognized and screening, treatment, intervention and patient education must be modified respectively. • Universal cytologic screening of all post pubertal women must be continued • Gardasil a quadrivalent vaccine against HPV16/18/6/11 received FDA approval in the USA for use in girls and women 9 – 26 years old.