Download
1 / 14
140 likes | 321 Views
MATERNAL-FETAL INTERACTIONS AND THE Rh BLOOD GROUP. Victoire N. Ndong Biology 327: Immunology. THE PLACENTA. HOW DOES THE FETUS STAY IMPLANTED IN THE UTERUS WITHOUT BEING REJECTED?. MEDAWAR’S THEORIES. The uterus is an “immunologically privileged site”

E N D
MATERNAL-FETAL INTERACTIONS AND THE Rh BLOOD GROUP Victoire N. Ndong Biology 327: Immunology
HOW DOES THE FETUS STAY IMPLANTED IN THE UTERUS WITHOUT BEING REJECTED?
MEDAWAR’S THEORIES • The uterus is an “immunologically privileged site” • The fetus is antigenically immature and the placenta is a neutral barrier. • There is immunosuppression during pregnancy • There will be a transfer of paternal antigen tolerance.
ANTIGENICITY OF THE PLACENTA • The outer layer of the placenta in contact with maternal blood never expresses MHC class II • The cytotrophoblast and the syncytiotrophoblast are MHC class I negative • NK cells could attack • The extravilloustrophoblast expresses HLA-C which is a classical polymorphic MHC class I gene product • HLA-C is less polymorphic than HLA-A and B • HLA-G is monomorphic and it’s expressed on the syncytiotrophoblast, causes apoptosis of Tcells.
IMMUNOSUPPRESSION • Indoleamine 2,3-deoxygenase (IDO) prevents tryptophan catabolism by T cell in placenta hence causing their inactivation and death. • Injection of IL-2 causes activation of CD8, CD4 and NK cells so to prevent this, the placenta secretes immunosuppressors like Th2 cytokines and the placenta recruits cells that secrete β2 transforming growth factor (TGF). • Increase in the number of rPg on T cells and NK cells after recognition of paternal antigens, and high progesterone level cause the secretion TJ6-RTF and PIBF which are potent immunosuppressors. • Fas interaction with Fasligand on Tcell causes apoptosis
IMMUNOTROPHISM • The size of the placenta increases with the number of pregnancies . • The placenta promote more implantation sites • Colony stimulating factors like IL-3 and GM-CSF produced by the mother are growth factors for the placenta so the placenta pushes for allorecognition by T cells to use their growth factors for it self. • Allorecognition causes IgG2 cytotoxic antibodies production and complement activation. • Placenta sends complement regulatory proteins like DAF (decay accelarating factor )and MCF (membrane cofactor protein)
PREGNANCY A Th2 PHENOMENON During pregnancy there is a suppression of Th1 responses by an increase of Th2 cytokines like anti inflammatory IL-10 IRENE ATHANASSAKIS et al.
Recent research • Recent research have shown that MIC (MHC class I chain) played a role in immune escape of tumors • MIC is a ligand for the activating site of the NK cell activating receptor NKG2D • So MIC-NKG2D is good for immune surveillance • However, soluble forms of MIC are produced by tumors maybe to act as a competitive inhibitors that block the recognition of the membrane bound MIC causing a downregulation of NKG2D • High levels of soluble MIC have been found in pregnancy serum
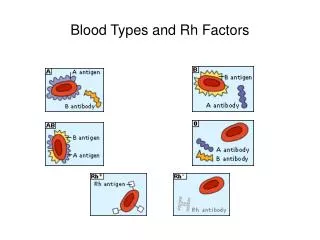
THE RHESUS BLOOD GROUP MODEL • Discovered by Landsteiner • More complex than the ABO blood group model • It has 54 antigens but the most important is the D antigen • Either the person expresses it or he doesn’t • Inheritance happens in a dominant way DD and Dd individuals are Rh+ and dd individuals are Rh- • Rh incompatibility can cause serious problems like Hemolytic disease of the newborn (HDN)
Hemolytic disease of the newborn • HDN happens when an Rh- mother is pregnant with an Rh positive baby • Fetal red blood cells enter maternal circulation causing immunization of the mother and production of IgG antibodies • The IgGs will cross the placenta and attack the fetal red blood cells • Antibody titers increase with time and for that reason the first pregnancy is the least at risk • There are many ways of preventing HDN
PREVENTION OF HDN • Intrauterine transfusion of compatible blood • Induction of labor right after pulmonary maturation • Injection of Rh immune globulin (RhIg) at 28 weeks of pregnancy and 72 hours after delivery.
SOURCES • Mincheva-Nilsson L, Nagaeva O, Chen T, Stendahl U, Antsiferoval, Mogren I, Hernestal J, Baranov V. Placenta-derived soluble MHC class I chain-related molecules down-regulate NKG2D receptor on peripheral blood mononuclear cells during human pregnancy: a possible novel immune escape mechanism for fetal survival. • Irene Athanassakis, VagiaFarmakiotis, and Lina Papadimitriou, “Uterine Cytokine Production During the Menstrual Cycle and Preimplantation Stages in Mice,” Developmental Immunology, vol. 7, no. 1, pp. 33-42, 1999. doi:10.1155/1999/67137 • Gérard Chaouat, INSERM, Clamart, France. Reproductive Immunology Standard Article • GérardChaouat, Hôpital A. Béclère, Clamart. Fetal–Maternal Immunological Relationships Standard Article




![[PDF] DOWNLOAD The Maternal Imprint: The Contested Science of Maternal-Fetal Effects](https://cdn7.slideserve.com/12531830/slide1-dt.jpg)