Download
1 / 29
461 likes | 2.74k Views
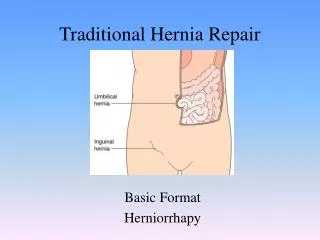
Parastomal Hernia Repair. C R Kapadia Airedale General Hospital. Parastomal Hernia. “Some degree of herniation around a colostomy is so common that this complication may be regarded as inevitable” Goligher. Parastomal Hernia. An Incisional Hernia related to an abdominal wall stoma.

E N D
Parastomal Hernia Repair C R Kapadia Airedale General Hospital
Parastomal Hernia “Some degree of herniation around a colostomy is so common that this complication may be regarded as inevitable” Goligher
Parastomal Hernia An Incisional Hernia related to an abdominal wall stoma. Particularly noticeable on tensing the abdominal wall muscles- coughing, sneezing, straining or standing.
Para Stomal Hernia Parastomal herniation is not uncommon and the management of a parastomal hernia is a common clinical dilemma. Once such a hernia is established, it is difficult to treat, and many operative factors have been claimed to influence its occurrence and many techniques of repair have been described. [Carne, Robertson and Frizelle]
Incidence of Parastomal Hernia 0 – 48% depending on type of stoma and length of follow up [Carne, PWG; Robertson, GM; Frizelle, FA. 2003] 20-25% Commoner in end colostomy [Devlin, 1982] 67% transverse loop colostomy [Nordstrum &Hulten, 1987]
Incidence of Parastomal Hernia 50% Colostomy [Nugent, 1999] 28% Ileostomy [Williams, 1990] 5-8% Urostomy [Rubin & Bailey1993]
Diagnosis History Examination - Standing - Lying Valsalva manoeuvre Digital examination of stoma CT Scan
Classification (Devlin) Interstitial Subcutaneous Intrastomal Peristomal
Risk Factors Extrinsic Emergency Surgery Location of Stoma Previous repair Intrinsic Age Obesity Wound Infection Smoking
Treatment Restore continuity of the intestine
Indications for Surgical Repair Strangulation Obstruction Fistula formation Ischaemia Pain Body Image - patient expectation
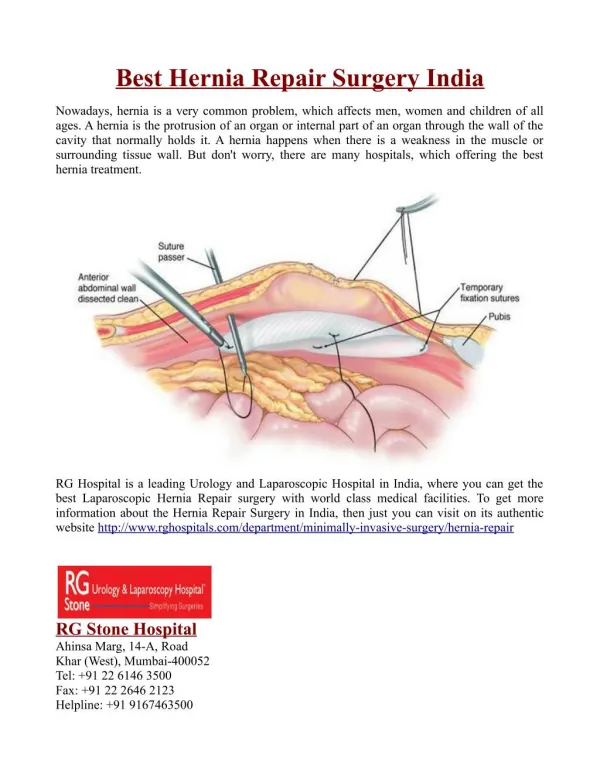
Choice of Surgical Procedures 1. Stoma Relocation 2. Local Tissue Repair 3. Prosthetic Repair - intraperitoneal - extraperitoneal - fascial onlay
Surgical Repair Increased infection rates Recurrence 39% [Reiger, 2004] Complications 57% [Hughes, 1999] Laparoscopic repair with mesh 10% recurrence[Le Blanc, 2004]
Cost Effectiveness Decreased: Chest infection Wound infection Adhesion complications Earlier recovery Shorter patient stay Better productivity
Advantages of Laparoscopy Direct magnified vision allowingidentification of fine anatomy Sharp precise dissection Reduction of operating time Reduced blood loss
Choice of Mesh 1. Compound polypropylene 2. e PTFE expanded polytetrafluoroethylene 3. Mixtures of absorbable and permanent fibres woven together to minimise the foreign body reaction
Pre op Post op
Pre op Post op
Pre op Post op
Pre op Post op
Patients Jan 2005 Female 76 years Colostomy 3 days Female 52 years Colostomy 5 days Male 68 years Colostomy 4 days Female 73 years Colostomy 4 days Female 68 years Urostomy 5 days Female 78 years Colostomy 6 days Female 68 years Ileostomy 4 days Male 58 years Ileostomy 5 days Male 49 years Ileostomy 4 days Female 65 years Colostomy 4 days
Follow Up Patients reviewed 3 monthly - 25 months No mesh related bowel erosion, fistulisation or adhesion formation observed 2 recurrences - further repair
Summary Faster recovery of bowel function Less morbidity Shorter length of hospital stay
Conclusion Parastomal herniae are common Associated with high morbidity Laparoscopic repair decreases post-operative pain Faster recovery Decreased overall morbidity Greater patient satisfaction