Download
1 / 24
240 likes | 263 Views
Explore the history, trends, and data quality issues of cervical carcinoma in situ collection in Michigan. Learn about reporting protocols, registry characteristics, and the implications of revised reportable lesion definitions. Discover the Michigan approach to surveillance methods.

E N D
Collection of Cervical Carcinoma In Situ in Michigan NAACCR Conference San Diego – 2009 Glenn Copeland, Michigan Cancer Surveillance Program Meg Watson, MPH, DCPC - CDC Mona Saraiya MD, MPH, DCPC - CDC
Topics to be Covered • History of Collection • Methods • Trends in Incidence • Data Quality Issues • Observations
Reporting of In Situ Cervical Lesions • Reportable Condition in Michigan • Michigan Followed SEER Definition in effect in 1984 • "Cancer" means all diagnosis with a behavior code of 2 (carcinoma in situ) or 3 (malignant primary site) ……..excluding basal, epithelial, papillary, and squamous cell carcinomas of the skin, but including carcinomas of skin of the vagina, prepuce, clitoris, vulva, labia, penis, and scrotum. Admin Rule 325.9051(1)(b)
Public Law 102-515 Enacted 10/24/1992 • Director of the Centers for Disease Control, may make grants to ….. statewide cancer registries in order to collect, for each form of in-situ and invasive cancer (with the exception of basal cell and squamous cell carcinoma of the skin), ….
NAACCR Working Group • Working Group on Pre-Invasive Cervical Neoplasia and Population-Based Cancer Registries - 1993 findings • Lack of common definition across registries • 3 tiered classification systems • Lack of uniformity-comparability • Other motivators • Cost of follow up due to age and survival • Treatment outcomes not pressing interest
Decisions to Stop Collection • NAACCR Working Group • Recommended against • Must stop collection effective on 1/1/1996 • “unless there is strong local need and interest and sufficient resources are available to collect all [high-grade squamous intraepithelial lesions] and its equivalent terms” • NPCR-CDC • May not use CDC funds for surveillance of CIS
Reasons to Continue • Reporting in Place • Metro Detroit SEER to Continue Collecting • Ad Hoc Advisory Committee Recommendation • Considerable Epidemiological Interest • One of few cancers with effective intervention • Cervical Cancer Advisory Committee • Of interest to cervical cancer control
Definition of Reportable Cervical Precancerous Lesions through 2008 • Reportable • Diagnoses of CIS or AIS • Diagnoses of CIN III with or without CIS • Diagnoses of HGSIL with or without CIS • Not Reportable • Diagnoses of CIN I or CIN II • Diagnoses of CIN III with severe dysplasia • Diagnoses of HGSIL with moderate or severe dysplasia
Systems for Classifying Cervical Lesions From Camilleri G., Blundell R. Research Journal Medical Sciences 3(1): 4-11, 2009
Characteristics of Michigan Registry • Statewide and Population Based • Began in 1985 • Passive Reporting • Hospital and Laboratory Reporting • Metropolitan Detroit SEER Registry • Captures 40-42 percent of Michigan cases • 58,000 Cases Annually • CDC/NPCR Funding Support since 1995 • App 3,000 Pre-invasive Cervical Lesions Annually • 5% of total cases
Number of Facilities Reporting In Situ Cervical CancersMichigan Resident Cases, 2000-2006
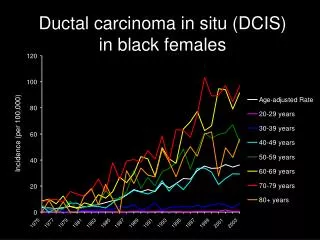
Copeland G, et al Total burden and incidence of in situ and invasive cervical carcinoma in Michigan, 1985-2003; Cancer Volume 113, Issue S10, Pages 2946-2954
Copeland G, Datta SD, Spivak G, Garvin AD, Cote ML.Total burden and incidence of in situ and invasive cervical carcinoma in Michigan, 1985-2003; Cancer Volume 113, Issue S10, Pages 2946-2954
Copeland G, Datta SD, Spivak G, Garvin AD, Cote ML.Total burden and incidence of in situ and invasive cervical carcinoma in Michigan, 1985-2003; Cancer Volume 113, Issue S10, Pages 2946-2954
Copeland G, Datta SD, Spivak G, Garvin AD, Cote ML.Total burden and incidence of in situ and invasive cervical carcinoma in Michigan, 1985-2003; Cancer Volume 113, Issue S10, Pages 2946-2954
Data Quality Issues • Collecting Cases not Required by ACOS • Incorporate in training • Emphasize during quality assurance efforts • High Proportion of Laboratory Only Reporting • Affects demographic completeness • Problem of Cytology Findings • Generates questions on reportability • Persistent Drift in Pathology Diagnostic Terms • HGSIL is very rare as pathology • Ongoing Validation Study • Early findings are good case-finding and low misreporting
Revised Definition Reportable Cervical Lesions • Reportable • Diagnoses of CIN III, CIS, or AIS • A Diagnosis of Severe Dysplasia • Not Reportable • Diagnoses of CIN I, CIN II or “CIN II/III” • High-grade SIL
CIN III Surveillance MethodMichigan Approach • Rapid Case Ascertainment • 30 days from diagnosis • Hard copies of positive lab reports • Hospitals and labs • Electronic lab reports • Modified AIM in selected labs • Complete Abstract • 3 to 6 months from diagnosis • Primarily Hospitals • Triggers follow up
Michigan CIN III Surveillance- Rapid Case Ascertainment 7/1/2008 - 3/19/2009
Data can Translate into Priorities • Cervical Cancer Implementation Objective 1: By 2011, reduce rates of cervical in-situ Cancer among women aged 20 to 39 years by 10%. Strategies • Targeted prevention messages • Increase HPV Vaccination Levels • Increase Plan First Enrollment • Increase Women Served by BCCCP/Family Planning • Promote Appropriate PAP testing in Minority Women • Encourage use of Provider Client Reminder Systems
Conclusions • Reporting of in situ cervical lesions is practical • Relatively efficient and reliable • Requires a solid collaborative relationship with facilities • Data yields meaningful information • Evaluation of trends informative • Useful in measuring success of screening • Can inform cancer control policy • Surveillance of CIN III is appropriate • Erosion of HGSIL into pathology report is negligible • CIS no longer separable from Severe Dysplasia • HPV vaccine establishes a new interest/value to data