Download

1 / 40
420 likes | 566 Views
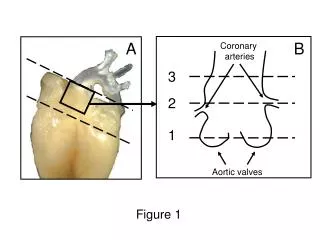
Coronary Artery Anomalies: Classification and ECG-gated Multi–Detector Row CT Findings with Angiographic Correlation1.

E N D
Coronary Artery Anomalies: Classification and ECG-gated Multi–Detector Row CT Findings with Angiographic Correlation1 So Yeon Kim, MD, Joon Beom Seo, MD, Kyung-Hyun Do, MD, Jeong-Nam Heo, MD, Jin Seong Lee, MD, Jae-Woo Song, MD, Yeon Hyeon Choe, MD, Tae Hoon Kim, MD, Hwan Seok Yong, MD, Sang Il Choi, MD, Koun-Sik Song, MD and Tae-Hwan Lim, MD
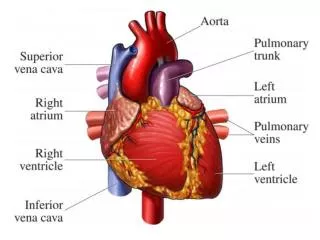
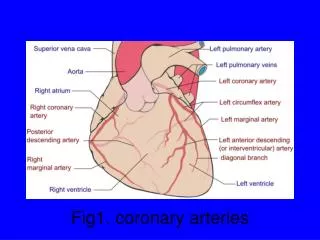
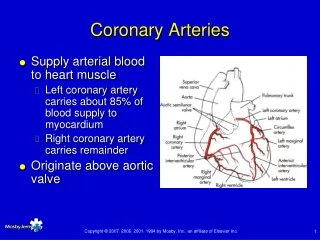
The four main coronary arteries evaluated at CT • Right coronary artery (RCA) • Left main coronary artery (LCA) • Left anterior descending (LAD) artery • Left circumflex (LCx) artery.
"circle and half-loop" model has been introduced to illustrate the anatomic relationships among these arteries. The circle consists of the RCA and the LCx artery, whereas the half loop is formed by the LAD artery and the posterior descending artery (PDA)
Dominant coronary artery • Artery crosses the crux of the heart and gives off the posterior descending branches is considered to be the dominant coronary artery. • 85% the RCA crosses the posterior interventricular groove and gives rise to the posterior descending branches (right dominance) • 7%–8% the LCx artery crosses the interventricular groove and gives rise to branches to the posterior right ventricular surface (left dominance) • Remaining 7%–8%, the inferior interventricular septum is perfused by branches from both the distal RCA and the distal LCx artery (codominance)
RCA • RCA arises from the anterior right coronary sinus , somewhat inferior to the origin of the LCA. The RCA passes to the right of and posterior to the pulmonary artery and then downward in the right atrioventricular groove toward the posterior interventricular septum. • In more than 50%, the first branch of the RCA is the conus artery, some has a separate origin directly from the right coronary sinus . • The second branches : the sinoatrial node artery and several anterior branches that supply the free wall of the right ventricle. • The branch to the right ventricle at the junction of the middle and distal RCA is called the acute marginal branch. • The distal RCA divides into the Posterior Descending Artery (PDA) and Posterior left ventricular Branch (PLB) = right dominant anatomy .
the RCA (arrow) arising from the right sinus of Valsalva and coursing in the right atrioventricular groove toward the posterior interventricular septum. • A = aorta • PA = pulmonary artery. • The conus artery and the sinoatrial node artery were too small to be seen in this case
The caudal course of the proximal RCA (arrow),gives off an acute marginal branch (arrowheads) to the right ventricle. • distal RCA divides into the PDA (straight arrow) and PLB(Posterior left ventricular branch arrowheads). • The PDA courses in the posterior interventricular groove, parallel to the middle cardiac vein (curved arrow).
LCA • The LCA arises from the left posterior coronary sinus, is 5–10 mm long, and does not vary in diameter. • The LCA passes posterior to the pulmonary trunk and bifurcates into the LAD and LCx arteries. • Occasionally, the LCA trifurcates into the LAD and LCx and the ramusintermedius(RI). • The ramusintermedius has a course similar to that of the first diagonal branch (D1) of the LAD to the anterior left ventricle. • The LAD artery passes to the left of the pulmonary trunk and turns anteriorly to the anterior interventricular groove toward the apex. • It provides the diagonal branches ( D1,D2,D3) to the anterior free wall of the left ventricle and the septal branches to the anterior interventricular septum. • The LCx artery courses in the left atrioventricular groove and gives off obtuse marginal branches( OM1,OM2) to the lateral left ventricle. • In a left dominant or codominant anatomy, the LCx artery gives rise to the PDA or posterior left ventricular branches /PLB .
The LCA (curved arrow) arising from the left sinus of Valsalva and trifurcating into the LAD artery (thin straight arrow), the LCx artery (thick straight arrow), and the ramus intermedius (arrowhead), which takes a course similar to that of the first diagonal branch. The LAD artery then gives rise to diagonal branches (short arrows) to the anterior free wall of the left ventricle.
The LAD artery (long thin arrows ) courses along the anterior interventricular groove. The LCx artery (long thick arrow ) courses in the left arterioventricular groove. Obtuse marginal branches (arrowheads) and diagonal branches (short arrows) are also seen.
ANOMALY CORONARY ARTERY • 1. Anomaly of origin : HIGH TAKE OFF • 2.Multiple Ostia • 3.Single coronary artery • 4. Anomalous Origin of the Coronary Artery from the Pulmonary Artery (ALCAPA) • 5.Origin of the Coronary Artery or Branch from the Opposite or Noncoronary Sinus and an Anomalous Course. • 6. Bridging myocardium • 7.Duplicated LAD • 8. Coronary artery fistula
Anomalies of Origin • High Takeoff.— refers to the origin of either the RCA or the LCA at a point above the junctional zone between its sinus and the tubular part of the ascending aorta , both coronary ostia were situated above the sinotubular junction in 6% of randomly selected adult hearts. • High take-off usually presents no major clinical problems, but it may cause difficulty in cannulating the vessels during coronary arteriography. • Selective intubation of the coronary artery may be extremely difficult, especially when the RCA is anomalously located high over the left coronary sinus .
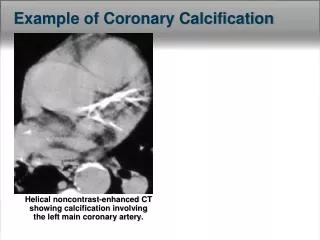
High takeoff of the RCA in a 55-year-old man. the RCA demonstrates a high take-off (arrow) above the sinotubular junction. Atherosclerotic change of the RCA with calcified plaque is also demonstrated.
Multiple Ostia • In multiple ostia, typically either the RCA and the conus branch arise separately , or the LAD and LCx arteries arise separately with no LCA . • An aberrant conus artery arising separately from the RCA is particularly at risk for injury from ventriculostomy or other maneuvers performed during heart surgery . • Separate ostia of the LCA and LCx artery may occur in a small percentage (0.41%) of individuals with otherwise normal anatomy . Although multiple ostia represent a technical difficulty for the angiographer, they may also allow alternate collateral sources in patients with proximal coronary artery disease
Multiple ostia with separate origins of the RCA and conus branch in a 60-year-old man. Coronal oblique MIP image shows separate ostia of the RCA (curved arrow) and conus branch (straight arrow) from the right coronary sinus.
Multiple ostia with separate origins of the LAD and LCx arteries in a 50-year-old man. separate ostia of the LAD (straight arrow) and LCx (curved arrow) arteries. A = aorta, PA = pulmonary artery.
Single Coronary Artery • only one coronary artery arises with a single ostium from the aortic trunk . • This is an extremely rare congenital anomaly that is seen in only 0.0024%–0.044% of the population . • A single coronary artery may either follow the pattern of a normal RCA or LCA, divide into two branches with distributions of the RCA and LCA, or have a distribution different from that of the normal coronary arterial .
Single coronary artery in an 80-year-old man. one coronary artery arising from the left coronary sinus (arrowhead). Note that the RCA (arrow) courses between the aorta (A) and the pulmonary artery (PA).
Single coronary artery in a 55-year-old man. • an anomalous origin for the RCA (curved arrow), which arises from the LAD artery (straight arrow) and courses anterior to thepulmonary artery (PA). A = aorta. • Coronary angiogram shows the anomalous origin of the hypoplastic RCA (curved arrow) from the LAD artery (straight arrow).
Anomalous Origin of the Coronary Artery from the Pulmonary Artery • Anomalous origin of the coronary artery from the pulmonary artery(ALCAPA) is one of the most serious congenital coronary arteryanomalies. • Most affected patients show symptoms in infancyand early childhood. • In the most common form of this disease,the LCA arises from the pulmonary artery and the RCA arisesnormally from the aorta (Bland-White-Garland syndrome). • Coronary angiography usually helps confirm the diagnosisof ALCAPA and demonstrates collateral circulation between theRCA and LCA and a coronary "steal" phenomenon into the pulmonaryartery
Bland-White-Garland syndrome in a 29-year-old woman. : • A dilated RCA (arrow) and the LAD artery with multiple collateral vessels at the right ventricular wall (arrowheads)
Origin of the Coronary Artery or Branch from the Opposite or Noncoronary Sinus and an Anomalous Course. • The four recognized patterns of an anomalous origin of a coronaryartery from the opposite or noncoronary sinus are: (a) the RCAarising from the left coronary sinus, (b) the LCA arising fromthe right coronary sinus. (c) the LCx or LAD artery arisingfrom the right coronary sinus. (d) the LCA or RCA (or abranch of either artery) arising from the noncoronary sinus. interarterialcourse betweenthe aorta and the pulmonary artery carries a high risk for sudden cardiac death(malignant annomaly)
Anomalous of the coronary artery may be found incidentally in 0,3-1% of healthy individuals. (SY KIM et al, radiographic 2006 ;26 : 317-333) • Classification coronary artery anomalies can be divided according to its : origin course and termination.
An anomalous origin of the right coronary artery from the left aortic sinus was first described in 1948 by White and Edwards. • There are 3 subtypes based on the anatomic course of the artery: 1. course posterior to the aorta (retroaortic), 2. between the ascending aorta and pulmonary trunk (interarterial) 3. anterior to the pulmonary trunk The interarterial subtype has been reported to be associated with angina pectoris, myocardial infarction, or sudden death ( 15%) in the absence of atherosclerosis ,also known as “malignant”anomalous.
Verious type Anomalous of single coronary artery PA rca PA rca
illustrate an LCA anomalously arising from the right coronary sinus (R) and four anomalous courses: A. interarterial (between the aorta and the pulmonary artery [PA]) , B. retroaortic , C. prepulmonic , and D. septal (subpulmonic [beneath the right ventricular outflow tract]) . L = left coronary sinus, N = noncoronary sinus.
RCA arising from the left coronary sinus and taking an interarterial course in a 44-year-old man. both the RCA (straight arrow) and the LCA (curved arrow) originating from the left coronary sinus. The RCA courses between the pulmonary artery (PA) and the aorta (A). Note the slit-like ostium (arrowhead) of the RCA.
LCA arising from the right coronary sinus and taking a prepulmonic course in a 50-year-old man. The LCA (arrows) originating from the right coronary sinus and taking a prepulmonic course, passing anterior to the pulmonary artery (PA). Oblique MIP image shows the separate origins of the LCA (arrows) and RCA (arrowhead) from the right coronary sinus, as well as the prepulmonic course of the LCA.
LCx artery arising from the right coronary sinus and taking a retroaortic course in a 45-year-old woman. The LCx artery (straight arrow) originating from the right coronary sinus and passing behind the aorta (A). The RCA (curved arrow) demonstrates its normal origination from the right coronary sinus. PA = pulmonary artery.
LAD artery arising from the right coronary sinus and taking a septal (subpulmonic) course in a 65-year-old man. • Both the LAD artery (long straight arrow) and the RCA (curved arrow) originating from the right coronary sinus. • The LAD artery takes an intramuscular course beneath the right ventricular outflow tract (removed with manual editing). • The LCx artery (short straight arrow) demonstrates its normal origination from the left coronary sinus. • A = aorta. (b)
Myocardial Bridging • Myocardial bridging is caused by a band of myocardial muscle overlying a segment of a coronary artery. • It is most commonly localized in the middle segment of the LAD artery • In some cases, myocardial bridging is responsible for : • angina pectoris • myocardial infarction • life-threatening arrhythmias • even death
Myocardial bridging in a 50-year-old man. During diastole and systole
Duplication of Arteries • Duplication of the LAD in normal hearts occur in 0.13%–1% of the general population. • Duplication of the LAD artery consists of a short LADartery, which courses and terminates in the anterior interventricularsulcus without reaching the apex, and a long LAD artery, whichoriginates from either the LAD artery proper or the RCA, thenenters the distal anterior interventricularsulcus and coursesto the apex . • The LAD artery is the mostimportant coronary artery in bypass graft surgery,the radiologist should be aware of the possibility of duplicationof the LAD artery so that the patient can forewarnthe cardiac surgeon of the importance of achieving successfulmyocardial revascularization; otherwise, there is a risk ofincorrect placement of the arteriotomy . • Duplication ofthe LAD artery should not be confused with an LAD artery anda diagonal branch running parallel to each other. • Such a paralleldiagonal branch does not reenter the anterior interventricularsulcus and take over the course of the distal LAD artery, asdoes the long anterior LAD artery .
Duplication of the LAD artery in a 47-year-old man. a dual LAD artery coursing along the anterior interventricular groove. Although the short LAD artery (short straight arrow) remains and terminates in the anterior interventricular groove, the long LAD artery (long straight arrow) reenters the groove from the anterior wall of the left ventricle. The diagonal branch (curved arrow) does not take this course. On a coronary angiogram, the origination of the septal branches (arrowheads) from the two arteries (arrows) proves that the arteries represent a dual LAD artery, not diagonal branches.