Download
1 / 60
600 likes | 742 Views
Basics of Dementia and Alzheimer’s Disease. Shelly Zylstra Northwest Regional Council zylstra@dshs.wa.gov. Definition of Dementia. An acquired intellectual deterioration which affects at least two areas of cognitive function.

E N D
Basics of Dementia and Alzheimer’s Disease Shelly Zylstra Northwest Regional Council zylstra@dshs.wa.gov
Definition of Dementia • An acquired intellectual deterioration which affects at least two areas of cognitive function. • In the past, commonly referred to as senility or “hardening of the arteries”
Memory Orientation Language Judgement Perception Attention Ability to perform tasks in sequence Cognitive Functions
Dementia is Not Normal Aging 20 year old brain 80 year old brain
Causes of Dementia • Causes of dementia • 47.7% Alzheimer’s • 10.0% Alcoholic dementia • 9.4% Vascular dementia • 6.0% Normal pressure hydrocephalus • 4.8% Intracranial masses (tumors) • 2.9% Huntington’s disease • 2.4% Drug toxicity • 1.7% Post-traumatic • 6.7% Pseudo-dementia
Intoxications Infections Metabolic disorders Depression Medication Problems Brain tumors Head injuries Normal pressure hydrocephalus Dehydration Reversible Dementias
Alzheimer’s disease Multi-Infarct Dementia Parkinson’s disease Lewy Body disease Creutzfeldt-Jakob disease Pick’s disease Huntington’s disease AIDS dementia complex Progressive aphasia Irreversible Dementias
Dementia of the Alzheimer’s-type (DAT) • Diagnosing DAT • Usually diagnosed by process of elimination • MRI shows enlarged ventricles and widening in folds of the cerebral cortex
DAT: Clinical features • Very gradual onset • Picture may differ from person to person • Gradual withdrawal from active engagement with life • Narrowing social activities and interests • Lessening of mental alertness and adaptability • Lowering of tolerance to new ideas and changes in routine • Thoughts and activities may be selfish or childlike
DAT: Clinical features • Messiness • Impaired judgment • Agitation • Periods of confusion • Terminal stages: person is in a vegetative state • Psychopathological symptoms are transitory and inconsistent • Sometimes paranoia
Vascular dementia • Clinical picture looks like DAT (increasing incidence with age) • Multiple small strokes cumulatively destroy neurons over an ever expanding brain area • Defective areas get soft over time • Less common than DAT, but may be more common in Indian Elders • May be associated with more severe behavioral complications such as violence • Increasingly vulnerable to sudden death
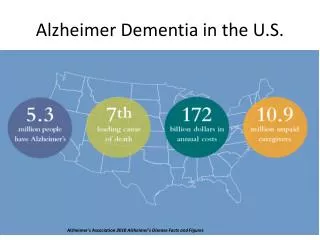
Prevalence of Alzheimer’s Disease • Over 4 million Americans plus their families • Number doubles every 5 years after age 65 • Numbers may triple by 2050 • 1/10 people over age 65 in USA • 5/10 people over age 85 in USA • 30-40% of nursing home patients have DAT
Stages of Alzheimer’s disease FunctionEarly Stage Memory Routine loss of recent memory Language Mild aphasia (word finding difficulty) Orientation Seeks familiar and avoids unfamiliar Motor Some difficulty writing and using objects Mood Apathy & depression ADL’s Needs reminders with some ADL’s
Stages of Alzheimer’s disease FunctionMiddle Stage Memory Chronic, recent memory loss Language Moderate aphasia Orientation May get lost at times, even inside the home Motor Repetitive actions, apraxia Mood Possible mood and behavioral disturbances ADL’s Needs reminders and help with most ADL’s
Stages of Alzheimer’s disease FunctionLate Stage Memory Mixes up past and present Language Expressive and receptive aphasia Orientation Misidentifies familiar persons and places Motor Bradykinesia, at risk for falls Mood Greater incidence of mood and behavioral problems ADL’s Needs reminders with all ADL’s
Stages of Alzheimer’s disease FunctionTerminal Stage Memory No apparent link to past or present Language Mute or few incoherent words Orientation Oblivious to surroundings Motor Little spontaneous movement, dysphagia, myoclonus, seizures Mood Completely passive ADL’s Requires total care
Treatment of Alzheimer’s Disease • Delay onset • Slow rate of progression • Treat primary symptoms (cognitive) • Treat secondary symptoms (behavioral)
Care of Persons with Alzheimer’s disease • Create a supportive atmosphere • Structure appropriate activities & routine • Design “dementia friendly” environments • Facilitate peer groups (for emotional support & shared activities)
Help for Family Caregivers • Offer education, training and consultation • Promote respite services; e.g.- adult day care, companion • Offer individual and family counseling • Encourage participation in support groups
The Basics of Good Communication with DAT • Rules of communication between two cognitively intact persons ( a 2-way street) • When one person has AD there is no longer an even exchange • Setting the right tone
Communication Changes • Early stage: Difficulty finding the right word, repetitiveness & keeping pace with others • Middle stage: Increased difficulty with speaking correctly & comprehending language of others • Late stage: Vocabulary reduced to a few words or phrases; increased need for nonverbal cues • Terminal stage: Mute or occasional word/phrase
Similar Functions Different Locations Seeing Words Speaking Words Hearing Words Seeing Words Thinking Words
Approaches of Others • Unrealistic expectations • Communication is key - verbal means - non-verbal means
Emotional Stressors • Diminished self-esteem • Fear related to the disease • Low frustration tolerance
Medications Pain Insomnia/fatigue Infections/illness Dehydration and malnutrition Constipation Poor vision and hearing Medical Stressors
Environmental Stressors • Stimulation - too much or too little • Physical design - helps and hindrances • Familiarity- cues & labels
When You Speak • Make the setting free of distractions • Gain attention, make eye contact, be aware of body language • Provide orienting information
Use short, simple sentences Use familiar and concrete words Break down tasks into steps Avoid open-ended questions Help reduce choices Language that Works
Trouble Understanding • Active listening • Focus on word or phrase that may have meaning • Respond to the emotional tone • Try to stay calm and be patient • Ask family members for clues
Trouble Being Understood • Allow enough time • Give a visual demonstration • Evaluate complexity of task • Change the subject if necessary
Things to Avoid • Don’t argue • Don’t give strict orders • Don’t be condescending • Don’t ask questions requiring detailed responses • Don’t talk about people in front of them • Don’t bother asking, “Do you remember?” in regard to recent events
Validate their Goodness! • Give them the gift of a one-way conversation. • Eat lunch with them. Don’t feed them. • Discuss your day. • Ask about their life when they were 10. • Don’t try to orient. Their reality is different from the present.
“While the majority of the attention to nutrition and Alzheimer’s Disease and dementia is related to cause and effect of specific nutrients or environmental concerns, the most time-tested nutritional aspect is what people with Alzheimer’s Disease are eating for dinner.” Zylstra, 1998
Goals of Nutrition in Alzheimer’s • Maintain weight • Individual more important than weight • Protect muscles to promote independence • Enhance immune function • Promote good bowel health • Good hydration • Medication management--prevent interactions, manage side-effects
Barriers to Good Nutrition Early Illness • Memory loss can lead to over- or under-eating. • Inability to prepare appropriate meals. • Food-born illness from improper food handling. • Depression/medications affect appetite. • Eating out can be embarrassing for family. • Begin to make changes for later illness now.
Solutions to Early Problems:Forget to eat… • Look for signs that food is not eaten…food taken to room from dining room and forgotten, scraps in garbage, food containers in refrigerator. • Provide snacks with activities and cue using smells--bread, cookies. • Watch for weight changes.
Solutions to Early Problems:Food Handling… • Food born illness can be an early warning sign of dementia. Food needs to be kept cold or hot and food-contact surfaces sanitized. • Microwave ovens are a mystery to many with dementia. • Breadbox? Pie Safe? Cake Keeper? • Automatic turn-off appliances can be useful. • Look into bad odors! Watch food supplies closely for old food which is unsafe to eat.
Solutions to Early Problems:Other Issues… • Depression can be associated with dementia at every stage of the disease. • Eating out can be embarrassing. • Medications used with dementia and depression can affect appetite and cause dry mouth which makes eating and swallowing difficult. • Educate family members about “Companion Cards” to prevent isolation.
Barriers to Good Nutrition Middle-stage illness • Prevent dehydration. • Respond to appetite changes. • Watch for poisons. • Visual perception can change. • Choice can be overwhelming. • Watch oral condition and care. • Watch for agitation and confusion. • Motor planning skills decrease (apraxia).
Solutions to Middle Problems:Dehydration… • Thirst perception may be seriously impaired. • Fluids should be offered every two hours. Broth Ice Cream Juice Popsicle's Jell-O Flavored water • Never restrict fluids to eliminate incontinence. Dehydration can cause incontinence by increasing confusion and causing urinary tract infection which increases urinary urgency. • Make “tea time” a regular social occasion.
Solutions to Middle Problems:Appetite Changes… • Appetite sensors can be impaired. • May not realize hunger and not eat regularly. • May not be able to feel satiety and may eat continuously (hyperphagia). • Offer snacks which are nutrient dense and easy to fix and eat--cheese and crackers, supplements. • Keep low calorie snacks around if weight gain is a problem. • Use other activities to distract attention from food...
Solutions to Middle Problems:Poisons and Inedibles… • Take precautions so that a confused person does not have access to everyday items which could be poisonous. • Common items which are eaten include soap, potting soil, paper napkins or Styrofoam cups, toothpaste and mouthwash or medications including vitamin pills. • It is important to document non-food items which are preferred and get this information from Respite clients.
Solutions to Middle Problems:Perception Changes… • It is sometimes difficult to discern food on plates. • Simple, unpatterned plates are best. • Table linens can be disturbing, if busy. Get plain non-skid placemats which contrast with dishes. • Playing with food is usually a sign of agitation or frustration or can mean physical problem. • Offer one utensil or one food at a time (tell families). • Watch mixtures! Component parts can prevent choking, and improve intake!
Solutions to Middle Problems:Dental Health… • Buy SOFT toothbrushes! • Be certain to have regular dental checkups to be certain that teeth or dentures are in good repair. • Supervise dental hygiene to assure quality brushing and be certain that products are not swallowed. • Dental problems can cause agitation, catastrophic behavior, and failure to thrive. Catch it early!!
Solutions to Middle Problems:Agitation/Confusion… • Minimize distractions at mealtime--no TV, sit with person, quiet conversation only, limit people at the table, pull shades, arrange mealtimes properly. • Eliminate emotional agitation by accepting people where they are. • Reality orientation doesn’t work in mid-/late-stage.
Solutions to Middle Problems: Agitation/Confusion… • Many difficult behaviors are the result of response to the perceived environment; chair seat color, floral rugs, patterns • Agnosia is the inability to recognize an object with the senses--visual, auditory, tactile. • Having someone to mimic can help eating behavior. • Be certain that all distracting physical needs are taken care of before eating (toilet, wet clothes)