Download
1 / 86
880 likes | 1.18k Views
Clinical Approaches to Anemia Presented by : Cheryl Morrow MD. I would like to acknowlege and thank the American Society of Hematology for granting permission to use their educational slides to illustrate this lecture. You will be able to access all of the images

E N D
Clinical Approaches to AnemiaPresented by: Cheryl Morrow MD
I would like to acknowlege and thank the American Society of Hematology for granting permission to use their educational slides to illustrate this lecture. You will be able to access all of the images that I will be using by going directly to the ASH Image Bank @ http://imagebank.hematology.org/ And type in the Slide number.
At the end of the program, the participant will be able to: • Name the common physiological responses and symptoms that occur in anemia • Name the laboratory tests that should be ordered to determine the degree of severity and type (etiology) of anemia with which a given patient is presenting. • List the likely cause(s) of anemia when provided the results of the patient’s laboratory tests for anemia • Based on an understanding of anemia etiology, name one recommended treatment option for each of the following anemia types: nutritional deficiency, CKD, blood loss anemia, autoimmune anemia, anemia due to bone marrow failure. Anemia: Course Objectives
Oxygen: the most essential element of human life - critical for: • Cellular respiration, growth and repair • Vital organ function: brain, heart, lung, kidneys, liver, nervous • Quality of life: movement, communication, senses, perceptions • Oxygen is critical but dumb ! (I’m a dumb ox) - it doesn’t know where it needs to go, how to get there, nor howmany of the crew are needed to get the job done at each location. • Hemoglobin has the esteemed jobs of both escorting and managing the entire crew of available oxygen molecules Anemia – So why do we care ?
The Proper Functioning of Hemoglobin requires: • adequate numbers (inadequate =anemia) • healthy molecules (Sickly =Hb S, C, thalassemia) • in a healthy environment (Sick = oxygen; CO ) Hemoglobin the Super Hero:
100% ___________________________________________________________ 65 35% oxygen dropped off 50 50% oxygen dropped off % Sat. 35 65% oxygen dropped off 0%___ 50 0 PaO2 mmHg 100 Left Shift: temp, pH, CO2, Hb F Right Shift: temp, pH, CO2 Oxygen-Hemoglobin Dissociation Curve
Functional definition of anemia: inadequacy of one’s hemoglobin, or the red blood cells that contain the hemoglobin, to transport and deliver adequate oxygen supplies to the tissues where it is needed. • Technical definition of anemia: • Males: hemoglobin < 14 g/dl; hematocrit < 40 % • Females: hemoglobin < 12 g/dl; hematocrit < 37%
Tired, Sleeping more • Loss of energy, weakness • Pale skin • Easy Fatigue • Tachycardia, esp. with exertion • New onset AF • Shortness of breath • Dizziness • Headache • Confusion, poor concentration • Angina Sx’s of Anemia = Sx’s of Hypoxemia
The RBC indices tell us about the Red Cell Physical Characteristics, and hemoglobin content: Think
So let’s talk about anemia: • Anemia develops when there is an imbalance between the productionand the loss/destructrion of RBC’s. • Anemia can also be caused by a genetic defect causing the production of faulty hemoglobin and/or RBC’s. • Thus, the causes of anemia can be classified as either … Low make, High take, Mistake!
BMP E-po. Defic Bone Marrow Ringed Sideroblasts MCV - Based Approach to Anemia Diagnosis : MCV <80 80 – 100 > 100 Microcytic Normocytic Macrocytic Ferritin & Iron Studies Reticulocyte Count Blood Smear Morphology Low Normal High Low Normal High -- HS PMN’s* + HS PMN’s IronThalassemia Anemia Anemia Acute Hemolysis Polychro- Target Vit B12 Defic. Hemoglobin- ChronicChronic Blood Chronic masia Cells Deficiency Anem. opathy Disease Disease Loss Bld.LossReticulo- Liver Folate Hemo- CRP,cytosis Disease Deficiency globin ESR LDH Electro- Sidero- Bilirubin Liver B12, phoresisblasticHaptoglobin ETOH Enzymes Folate Lead poisoning anemia Direct Anti- Abuse Levels, globulin test Hypothyroid MMA, Lead Bone Marrow Schilling Level Ringed sideroblastsMelodysplasia TFT’s Test * HS PMN’s= HypersegmentedPolymorphonuclear Neutrophils
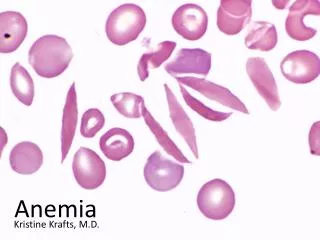
Microcytic Anemias . . . . “Anorexics love to ingest small” ( MCV< 70)
Case 1: Mrs. B is a 92 year old nursing home patient who, on routine lab testing, was found to have a hemoglobin of 9.0, and a hematocrit of 28.1. The patient’s aids note that she requires more assistance with ADL’s of late. She is weaker and seems more confused. Other Labs: WBC 6.9 (5-10) platelet 460 (150,000-400,000) MCV 70.5 (80-100) MCH of 22.5 (27.0-32.0) MCHC 32.0 (32-36) RDW was elevated at 17.8 (11.5-14.5) What is in the differential diagnosis? What do we do next?
Bone Marrow Ringed Sideroblasts MCV - Based Approach to Anemia Diagnosis : MCV <80 80 – 100 > 100 Microcytic Normocytic Macrocytic Ferritin (& Iron Studies) Reticulocyte Count Blood Smear Morphology Low Normal High Low Normal High -- HS PMN’s* + HS PMN’s IronThalassemia Anemia Anemia Acute Hemolysis Polychro- Target Vit B12 Defic. Hemoglobin- ChronicChronic Blood Chronic masia Cells Deficiency Anem. opathy Disease Disease Loss Bld.LossReticulo- Liver Folate Hemo- CRP,cytosis Disease Deficiency globin ESR LDH Electro- Sidero- Bilirubin Liver B12, phoresisblasticHaptoglobin ETOH Enzymes Folate Lead poisoning anemia Direct Anti- Abuse Levels, globulin test Hypothyroid MMA, Lead Bone Marrow Schilling Level Ringed sideroblastsMelodysplasia TFT’s Test * HS PMN’s= HypersegmentedPolymorphonuclear Neutrophils
Case 1 continued: Iron studies: Ferritin: 8 (10-250) LOW Serum Iron: 14 (35-150) LOW TIBC: 254 (250-450) NORMAL % Saturation: 6 (12-50) LOW
Case 1 continued: Iron studies: Ferritin: 8 (10-250) LOW Serum Iron: 14 (35-150) LOW TIBC: 254 (250-450) NORMAL % Saturation: 6 (12-50) LOW Diagnosis: Iron Deficiency AnemiaTreatment: Supplemental iron; Look for occult GI bleed
Case 2. Peter is a six year old boy who developed headaches, difficulty sleeping, stomach pain, weight loss, irritability and regression in school over the past several months. His mother, who is a single mom, usually works until 6 at night and the patient and his ten year old sibling are left alone in their apartment in the late afternoon until Mom returns. Labs: His Hb is 8,8; Hct is 26.2; His Ferritin was WNL. His other iron studies were within normal limitis.His peripheral blood film as follows:
Bone Marrow Ringed Sideroblasts MCV - Based Approach to Anemia Diagnosis : MCV <80 80 – 100 > 100 Microcytic Normocytic Macrocytic Ferritin (& Iron Studies) Reticulocyte Count Blood Smear Morphology Low Normal High Low Normal High -- HS PMN’s* + HS PMN’s IronThalassemia Anemia Anemia Acute Hemolysis Polychro- Target Vit B12 Defic. Hemoglobin- ChronicChronic Blood Chronic masia Cells Deficiency Anem. opathy Disease Disease Loss Bld.LossReticulo- Liver Folate Hemo- CRP,cytosis Disease Deficiency globin ESR LDH Electro- Sidero- Bilirubin Liver B12, phoresisblasticHaptoglobin ETOH Enzymes Folate Lead poisoning anemia Direct Anti- Abuse Levels, globulin test Hypothyroid MMA, Lead Bone Marrow Schilling Level Ringed sideroblastsMelodysplasia TFT’s Test * HS PMN’s= HypersegmentedPolymorphonuclear Neutrophils
Diagnosis: • The blue speckles seen on several RBC’s is Basophilic Stippling. • Basophilic stippling is seen in heavy metal poisoning, particularly lead poisoning, the thalassemias; and a few other conditions. • His blood lead level was 22 mg/dl (upper nl is 5 mg/dl for child) • Diagnosis was made: chronic lead poisoning caused by ingestion of paint chip fragments. • Treatment: hospitalized for IV chelation therapy with DMSA and returned to his baseline. Lead Poisoning
Case 3 HPI: A 42-year-old woman was referred for mild, chronic microcytic anemia discovered 18 years before. She c/o chronic fatigue that she has learned to live with. PE: was normal except for some generalized weakness. Labs: Hb 9.6 g/dL, MCV 73 fL, MHC 23 pg (27-32) RDW 27% (10.5-14.5). The WBC and platelet counts were WNL. Iron studies: ferritin 465 (10-252). Fe, % Sat are TIBC nl. Her peripheral smear follows:
Bone Marrow Ringed Sideroblasts MCV - Based Approach to Anemia Diagnosis : MCV <80 80 – 100 > 100 Microcytic Normocytic Macrocytic Ferritin (& Iron Studies) Reticulocyte Count Blood Smear Morphology Low Normal High Low Normal High -- HS PMN’s* + HS PMN’s IronThalassemia Anemia Anemia Acute Hemolysis Polychro- Target Vit B12 Defic. Hemoglobin- ChronicChronic Blood Chronic masia Cells Deficiency Anem. opathy Disease Disease Loss Bld.LossReticulo- Liver Folate Hemo- CRP,cytosis Disease Deficiency globin ESR LDH Electro- Sidero- Bilirubin Liver B12, phoresisblasticHaptoglobin ETOH Enzymes Folate Lead poisoning anemia Direct Anti- Abuse Levels, globulin test Hypothyroid MMA, Lead Bone Marrow Schilling Level Ringed sideroblastsMelodysplasia TFT’s Test * HS PMN’s= HypersegmentedPolymorphonuclear Neutrophils
Peripheral Smear showed a double population of RBC’s: one normal and one extremely microcytic and hypochromic. Very unusual need a bone marrow. • Bone marrow aspirate:35% of erythroid cells were ringedsideroblasts: nucleatederythroblastswith granules of (Prussian-blue stained) ironin perinuclearmitochondria • In sideroblastic anemia, the body/RBC has iron available but cannot incorporate it into hemoglobin. Ringed sideroblasts = Sideroblastic Anemia
Case 3: • X-linked sideroblastic anemia was confirmed by DNA sequencing on this patient. A skewed X-chromosome inactivation ratio explained the phenotype with two cell populations. Gender preval.: 1/3 women and 2/3 men. • AquiredSideroblastic anemia: myelodysplastic syndrome, ETOH abuse, lead poisoning, B6 defic., drugs (Isoniazid, linezolid, etc) • Treatment: Oral pyridoxine (B6) therapy for all types with varying effectiveness. In this real case, pyridoxine increased her Hb to 11.4; and peripheral films showed disappearance of the microcytic population. Diagnosis: X-Linked Sideroblastic Anemia
NormocycticAnemias . . . . “average men hunt burgers” (MCV 80-100)
BMP E-po. Defic Bone Marrow Ringed Sideroblasts MCV - Based Approach to Anemia Diagnosis : MCV <80 80 – 100 > 100 Microcytic Normocytic Macrocytic Ferritin & Iron Studies Reticulocyte Count Blood Smear Morphology Low Normal High Low Normal High -- HS PMN’s* + HS PMN’s IronThalassemia Anemia Anemia Acute Hemolysis Polychro- Target Vit B12 Defic. Hemoglobin- ChronicChronic Blood Chronic masia Cells Deficiency Anem. opathy Disease Disease Loss Bld.LossReticulo- Liver Folate Hemo- CRP,cytosis Disease Deficiency globin ESR LDH Electro- Sidero- Bilirubin Liver B12, phoresisblasticHaptoglobin ETOH Enzymes Folate Lead poisoning anemia Direct Anti- Abuse Levels, globulin test Hypothyroid MMA, Lead Bone Marrow Schilling Level Ringed sideroblastsMelodysplasia TFT’s Test * HS PMN’s= HypersegmentedPolymorphonuclear Neutrophils
Reticulocytosis: • Reticulocytes: immature RBC’s pushed out of the bone marrow early because of anemia. They stain “blue” because of nuclear fragments. These fragments show up better on a vital stain which enables counting of reticulocytes • Polychromasia: the bluish tint of the reticulocytes on a routine Wright’s stain, provides evidence of immature RBC’s • Example: Hemolytic disease of the newborn secondary to ABO incompatibility • Notice the polychromasia (causing an increase in MCV) • Notice the nucleated RBC
Case 4 A 58 year old, obese, diabetic female presents with c/o feeling exhausted. She states that over the past 1 month, she has gotten increasingly short of breath while walking from the parking lot to his office. Over the past one week, she has also experienced the sensation of her “heart pounding out of her chest” when walking back and forth to his car. When you ask her about pain, she admits to chronic back and joint pain for which she regularly takes ibuprofen with good relief. She denies dyspepsia, diarrhea, melena and hematochezia. She is post-menopausal. Her PE is normal. What is the Ddx ?
Case 4 continued: Relevant lab work is as follows: Na 135 WBC 7.6 MCV 92 K+ 4.4 Hb 8.2 MCH 29 (27-32) Cl 106 Hct: 24.5 Serum Fe normal CO2 24 Plt: 333 Ferritin normal BUN 64 Diff: normal Creat. 3.2 RBC morphology on next page. GFR: 19 Reticulocyte count: 0.4 (0.5-2.5) What kind of anemia does she have?
BMP E-po. Defic Bone Marrow Ringed Sideroblasts MCV - Based Approach to Anemia Diagnosis : MCV <80 80 – 100 > 100 Microcytic Normocytic Macrocytic Ferritin & Iron Studies Reticulocyte Count Blood Smear Morphology Low Normal High Low Normal High -- HS PMN’s* + HS PMN’s IronThalassemia Anemia Anemia Acute Hemolysis Polychro- Target Vit B12 Defic. Hemoglobin- ChronicChronic Blood Chronic masia Cells Deficiency Anem. opathy Disease Disease Loss Bld.LossReticulo- Liver Folate Hemo- CRP,cytosis Disease Deficiency globin ESR LDH Electro- Sidero- Bilirubin Liver B12, phoresisblasticHaptoglobin ETOH Enzymes Folate Lead poisoning anemia Direct Anti- Abuse Levels, globulin test Hypothyroid MMA, Lead Bone Marrow Schilling Level Ringed sideroblastsMelodysplasia TFT’s Test * HS PMN’s= HypersegmentedPolymorphonuclear Neutrophils
Case 4 • Answer: she has Anemia of Chronic Kidney Disease with acute on chronic renal failure secondary to NSAID use. • Treatment: Stop NSAIDS! Treat anemia with erythropoetin. Monitor kidneys closely
Case 5 HPI: A 21-year-old African-American woman presented for routine prenatal care for her second pregnancy. Her past medical history included normocytic anemia of uncertain etiology, for which she was treated with iron, during her first pregnancy. Her physical examination was unremarkable. Labs: hemoglobin, 9.4 g/dL; MCV 81 fl; RDW 15.3 WBC and platelet counts were WNL Electrophoresis/chromatography for. hemoglobinopathywere normal, Here is her periperal blood film:.
Hemolytic Anemia • Peripheral blood smear showed many elliptocytes, which is diagnostic of hereditary elliptocytosis(HE). • HEis caused by various gene mutations ultimately affecting the red cell cytoskeleton and membrane protein integrity Spontaneous hemolysis not mediated by Ab’s. • HEis seen in numerous ethnic groups; with incidence highest in west and central Africans. • Most patients with heterozygous HE are asymptomatic, although some may demonstrate hemolytic anemia and splenomegaly. • Other lab findings: haptoglobin, LDH, Indir. Bilirubin, direct antiglobulin test (DAT) is neg. b/c not Ab-mediated. • Treatment: Folic acid reduces hemolysis.
Case 6. HPI: A previously healthy 23 year old male college student was noted by his buddies to be pale, fatigued, and just not keeping up. His mother comes to visit and notes that he has lost 10 pounds over the past 1 month. She She wonders if he has been using drugs. She brings him to your office for evaluation. Lab tests reveal: WBC 11.8, Hb 8.3, Hct 26.0, MCV 96 What’s your Ddx? What questions do we need to ask him?
Case 6, continued: Upon your ROS, he reveals that he has had Multiple episodes of loose stool over the Past two months. When pressed, he admits That the stools have been maroon in color. Additional Labs: Na 148, K 3.2, CO2 16, BUN 32, Creat. 1.2 (BUN/Creat. Ratio 27). WBC 11.8, Hb 8.3, Hct 26.0, MCV 96 What’s your Ddx? What do we do next to confirm the dx?
BMP E-po. Defic Bone Marrow Ringed Sideroblasts MCV - Based Approach to Anemia Diagnosis : MCV <80 80 – 100 > 100 Microcytic Normocytic Macrocytic Ferritin & Iron Studies Reticulocyte Count Blood Smear Morphology Low Normal High Low Normal High -- HS PMN’s* + HS PMN’s IronThalassemia Anemia Anemia Acute Hemolysis Polychro- Target Vit B12 Defic. Hemoglobin- ChronicChronic Blood Chronic masia Cells Deficiency Anem. opathy Disease Disease Loss Bld.LossReticulo- Liver Folate Hemo- CRP,cytosis Disease Deficiency globin ESR LDH Electro- Sidero- Bilirubin Liver B12, phoresisblasticHaptoglobin ETOH Enzymes Folate Lead poisoning anemia Direct Anti- Abuse Levels, globulin test Hypothyroid MMA, Lead Bone Marrow Schilling Level Ringed sideroblastsMelodysplasia TFT’s Test * HS PMN’s= HypersegmentedPolymorphonuclear Neutrophils
Case 6, continued: Upon your ROS, he reveals that he has had Multiple episodes of loose stool over the past 2-3 weeks. When pressed, he admits That the stools have been loose and bloody. Additional Labs: Na 148, K 3.2, CO2 16, BUN 32, Creat. 1.2 (BUN/Creat. Ratio 27). WBC 11.8, Hb 8.3, Hct 26.0, MCV 96 His peripheral blood film is the next slide. What’s your Ddx? What do we do next to confirm the dx?