Download
1 / 26
510 likes | 1.59k Views
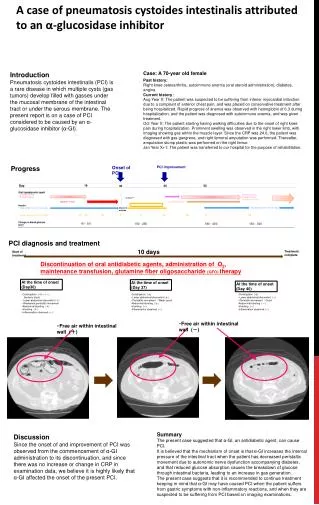
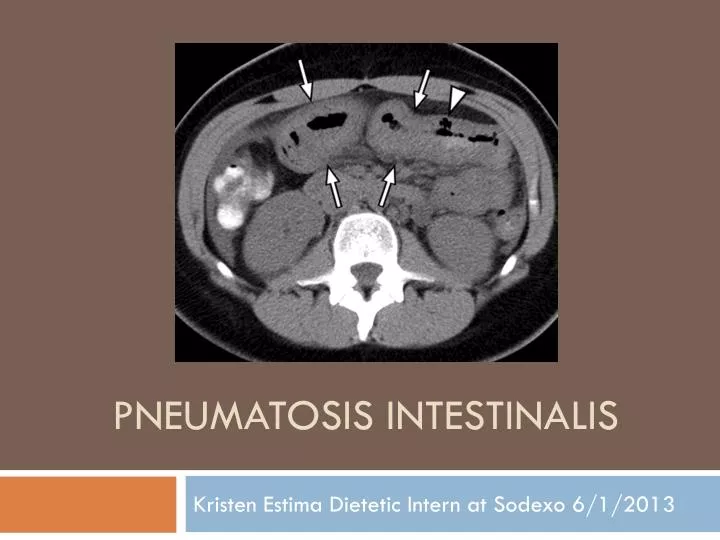
Pneumatosis intestinalis . Kristen Estima Dietetic Intern at Sodexo 6/1/2013. Definition . Pneumatosis Intestinalis (PI) or also known as Pneumatosis cysoides intestinalis- it’s characterized by the presence of small cysts of air in the intestines. Many cases of PI are asymptomatic

E N D
Pneumatosis intestinalis Kristen Estima Dietetic Intern at Sodexo 6/1/2013
Definition • Pneumatosis Intestinalis (PI) or also known as Pneumatosis cysoides intestinalis- it’s characterized by the presence of small cysts of air in the intestines. • Many cases of PI are asymptomatic • PI is a rare disease and its etiology is unknown.
Etiology theories • There are three etiology theories: • Mechanical theory • Bacterial theory • Pulmonary theory
Mechanical theory • Based on the explanation that that gas could be forced under pressure through a mucosal defect into the bowel. This could happen due to trauma, bowel obstruction, and surgery or simply due to an endoscopic procedure. • Most accepted theory!
Bacterial theory • Based on the invasion of bacteria into the bowel. In some animal experiments when bacterial was injected into the bowel, pneumatosis intestinalis resulted in some cases. • Antibiotics have led to the cure of PI, which leads researcher to believe that bacteria could play a major role in the disease process of PI.
Pulmonary theory • Based on the idea that the gas from a ruptured alveoli could travel though the mesentery into the bowel wall • Least accepted theory!
Forms of Pneumatosis Intestinalis • Idiopathic/primary form: characterized by the presence of multiple thin-wall cysts in the submucosa or subserosa of the gut. This form is usually diagnosed through radiography or endoscopy, as it’s usually asymptomatic and it occurs in 15% of cases • Secondary form (which is the most common) is often related to OPD (Obstructive Pulmonary Disease) and/or obstructive and necrotic gastrointestinal disease. Occurs in 85% of cases.
Symptoms of Pneumatosis Intestinalis • Diarrhea is mostly common but constipation is possible. • Vomiting • Blood in stool and emesis. • Abdominal Pain • Abdominal distention • Weight loss
Treatments of Pneumatosis Intestinalis • Hyperbaric Oxygen Therapy (may be enough to treat the collection of gas in patients who are asymptomatic)- oxygen is toxic for the anaerobic bacteria, which are responsible to the gas production in the bowel • Surgery/Laparotomy (If severe inflammation, metabolic acidosis and portal venous gas present). • Antibiotics- kills bacteria in the bowel.
Ischemic Colitis (IC) and P. Instestinalis • Pneumatosis intestinalis can result from an Ischemic Bowel. • IC can result from a bowel obstruction either caused by a tumor; hernias, diverticulitis, volvuli or adhesions. • Congestive congestive heart failure, intense physical activity, hypotension, and/or shock that result from the patient’s septic state or hypovolemiacan predispose the patient to IC. • Certain medications such as antibiotics, phentermine (appetite suppressant), chemotherapy, decongestants, diuretics, statins, illicit drugs, immunosuppressive drugs, anti-inflammatory drugs .
Gangrenous Bowel • Gangrenous bowel means tissue death • Main goal is to resuscitate the tissue, prevent further propagation of the blockage, prevent reperfusion injury and restore the blood flow as soon as possible. • The outcome for patients with gangrene ischemic bowel can be poor. • If bowel resection is performed, they often develop short-gut syndrome and therefore requite total parenteral nutrition or small bowel transplantation.
Medical Nutrition Therapy • Upon admission a patient is prescribed a NPO diet. • Enteral Nutrition seems to induce a reactive hypermetabolic response and reduce septic complications, and therefore improving the mucosal barrier function and decreasing the bacterial translocation( Jejunostomyprefered). • Supplementing fiber along with the enteral tube feeding may help prevent overgrowth of pathogenic bacteria, as well as helping in the prevention of septic complications.
Medical Nutrition Therapy • If patient shows signs of intolerance, total parenteral nutrition should be given as an alternative. • Elemental formulas have been shown to alter the micro-flora, and therefore, help with the resolution of PI. • Low-residue diet should be slowly initiated as the patient improves. • Supplementation of glutamine and antioxidants either through enteral feeding or through PO is beneficial as these are immunonutrients and improve the patient’s immune system. • ASPEN guidelines for critically ill patient should be followed.
Presentation of Patient • Caucasian • Age: 75 years old • Weight: 200lbs/90.7kg on admission • Height: 71 inches • BMI: 27.9 • Chief complaints: 10/10 abdominal pain, fever, diarrhea and vomiting for two consecutive days, nausea. Denied blood in stool or emesis. Onset of respiratory difficulty and arrived at the unit with severe shortness of breath.
Past Medical History • Hernia repair (2 months prior to admission) • Hypertension • High Cholesterol • Tonsillectomy • Carpal Tunnel disease • Atrial fibrillation • Smoker in the past (quit over 10 years ago) • Married, considers himself active and healthy and has great appetite at home.
Medications • Carvedilol (Coreg)- beta-blocker • Losartan Potassium (Cozar)- antihypertensive drug • Diltitiazem(Cardizem)- calcium channel blocker • Lovastatin (Mevacor, Altoprev)- HMG-CoA reductase inhibitor (statin) drug • Warfin (Coumadin)- is an anticoagulant drug. • Zofran (ondansetron)- is an antiemetic drug to prevent nausea and vomiting
Diagnosis Per MD impression: • 1)PneumatosisInstestinalis 2)Gangrenous bowel 3)Acute intestinal vascular insufficiency/ ischemic colitis. • Coagulopathy was present secondary to Coumadin/A-Fib. • Length of stay was 10 days, for which he spent five days in the Intensive Care Unit and two days on the telemetry floor.
Admission labs • Glucose: 100; BUN: 39 (high); Sodium: 143; Potassium: 3.5; Chloride: 105; C02: 26; Creat: 1.43. CK: 223 (high); CKMB: 11.0 (high); AST: 32; ALT: 32; Alkaline Phosphatase: 74; Amylase: 33; Lipase: 41; Calcium: 8.8; Iron: 13 (low); Phosphorus: 3.6; Magnesium: 2.1; Uric acid: 9.2 (high); Total Protein: 6.5; Albumin: 3.6; Triglycerides: 98; HDL: 34 (low); LDL: 64; Cholesterol: 121; WBC: 72; RBC: 2.69 (low), HGB: 8.4 (low); MCV: 91.4; MCH: 30.5; Neutro%: 73.9; Lymph%:13.3(low); Mono%: 11.5(high); Vitamin B12: 332; Folate: 20.7; Ferritin: 157.
Diagnostic Tests • CT of abdomen Pelvis without IV contrast– PI confirmed • Chest X-ray: revealed poor inspiratory effort. No acute pulmonary disease • Renal Ultrasound: revealed a 3.2cm left renal cyst. 2.2cm cyst in the hypoechoic area of the right kidney. • Ultrasound of Pelvis: foleycathether, bladder volume 217 cc, prostate 28cc, suspect ileus associated with infarction. • Abdomen X-ray: mild distention of the hepatic flexure but not transverse colon. Small bowel dilation observed.
Diagnostic Tests • Echocardiogram: showed mild pulmonary hypertension with dilated right ventricle. Normal left ventricular size and systolic function. • Thrombectomy performed: went in from the right femoral artery to the mesenteric to visualize arterial system (it was dying, no vascularization). Thrombectomy catheter prepped and flushed. Coronary injection filmed and reviewed. Second unit of Fresh Frozen Plasma (FFP) complete. Nitrogen given IA. Wire and cobra removed and third unit of FFP hung.
Prognosis • Cardiology report: Ischemic Bowel status post thrombectomy. Pt feels much better and abdomen is soft. Positive bowel movement and bowel sounds- bowel was revascularized,No resection needed. • Nephrologist: reports acute tubular necrosis. • PneumatosisIntestinalis resolved. Bowel movement is liquid and green from the contrast given. • C-diff negative: Imodium ordered to help with loose stool. • Hypertension controlled. A-Fib, high WBC but stable with no fever.
Nutrition care • First nutrition assessment was done two days after: admission: • Nutritional needs: • Calories: (2275-2548kcal); 25-28kcal/kg; 25x91kg= 2275kcal; 28x91= 2548kcal • Protein: (109-136g); 1.2-1.5g/kg; 1.2x91=109g; 1.5x91=136g • Fluid needs: (2275-2548ml) 1ml per kg. • Nutrition diagnosis: Inadequate oral intake related to GI distress as evidence by NPO x4days, not meeting needs. • Nutrition goals: 1) Initiate clear liquids by next assessment. 2) Meet >75% or more of Pt nutrient needs. • Dietetic Intervention: 1) when medically appropriate, initiate clear liquids. 2) Recommend MVI (standard vs. renal). • Monitor: Patient is at high nutrition risk. Monitor ability to initiate nutrition, weight, labs and progress to goals on follow-up in 3 days.
Nutrition care • Patient seen for follow-up: • Patient tolerating full liquids diet without nausea/vomiting. No abdominal pain. • Abdomen soft, non-tender, normal bowel sounds. Loose stool-present. • Abdomen soft, non-tender, normal bowel sounds. Loose stool-present. • 1) Recommend advancing diet to low-residuals when medically appropriate. • Monitor diet tolerance, plan of care, labs, weight and progress to goals on f/u in 3-4days.
Nutrition care • Patient seen for follow-up: • Patient is on a low-residue diet/ ½ NS with KCL. • Patient tolerating low-residue diet per RN, although diarrhea was noted in RN sheet. • Acute intestinal ischemia still present. Low magnesium noted- Mg sulfate ordered. • Patient reports good appetite and is tolerating diet advancement without abdominal pain. Loose stool improving with Imodium. • Monitor diet tolerance, labs, weight and plan of care on f/u in 3-4days.
Summary • This patient had a really good prognosis and outcome. • No enteral or parenteral nutrition was needed during hospitalization and patient tolerated diet progression well. • In addition, bowel resection was not needed, as the doctor was able to vascularize the necrotic tissue. • The patient was discharged on a low residue, 2g sodium, and low cholesterol diet per MD order. Patient’s weight and labs were stable on discharge.
References • Saber, Aly. "Pneumatosisintestinalis with complete remission: a case report." Cases journal 2 (2009): 7079.Dayal, Sanjeev, et al. "Extensive PneumatosisIntestinalis in Association With Celiac Disease: A Case Report." Journal of Medical Cases 2.2 (2011): 39-43. • Srivastava, Vivek, VaibhavPandey, and SomprakasBasu. "Intestinal Ischemia and Gangrene.” • McClave, Stephen A., et al. "Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (ASPEN)." Journal of Parenteral and Enteral Nutrition 33.3 (2009): 277-316. • Melis, Marcovalerio, Alessandro Fichera, and Mark K. Ferguson. "Bowel necrosis associated with early jejunal tube feeding: a complication of postoperative enteral nutrition." Archives of Surgery 141.7 (2006): 701. • Scaife, Courtney L., Jeffrey R. Saffle, and Stephen E. Morris. "Intestinal obstruction secondary to enteral feedings in burn trauma patients." The Journal of Trauma and Acute Care Surgery 47.5 (1999): 859. • Pronsky, Zaneta M., and Jeanne P. Crowe. Food Medication Interactions. Birchrunville, Penn.: Food-Medication Interactions, 2010. Print.