Download
1 / 42
420 likes | 557 Views
Hierarchy of Clinical Needs. Charlie Fairhurst Evelina Children’s Hospital Guy’s and St.Thomas’ Hospitals Kings Health Partners – Lambeth branch . South Thames Movement Service Evelina Children’s Hospital. What’s really most important in life. CONTENTS. Background

E N D
Hierarchy of Clinical Needs Charlie Fairhurst Evelina Children’s Hospital Guy’s and St.Thomas’ Hospitals Kings Health Partners – Lambeth branch
CONTENTS • Background • Abilities and Disabilities Basics of overall medical management • Development of Hierarchy of Clinical Need – needs of the child and family • Place of Pain and Nutrition within it • Summary / pitfalls
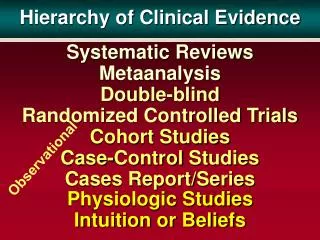
HIERACHY OF CLINICAL NEED WHY DO WE DO WHAT WE DO SOCIAL MODEL VS CLINICALNEED PAIN NON RECOGNITION AND MIS-MANAGEMENT
Impairment Physical Neurodisability Physical Causes Disability Functional problems Handicap Integration in society
Physical Neurodisability • Emergency care - medical stabilisation • Diagnosis • Long termManagement ~ • Child ~ Quality of life • Think holistically • Nutrition • Seizures / Spasms • Movement / Mobility / Posture • Management - Family & interdisciplinary support ~ Quality of life • Palliative Care
Service provision – problems in patient pathway • BIGproblems • Frequency of appointments • Numbers of people • Numbers of different professions • Different needs of individual child
Multidisciplinary management - services for paediatric neurodisability • What is the best clinical practice for each individual? • How can we help the team reflect on our attempts to deliver this? • How can we help us all to understand what is needed?
Was the child being asked to perform above their clinical / developmental ability? • Was the goal setting for the child appropriate? • Was their sufficient regular re-appraisal of each child’s need?
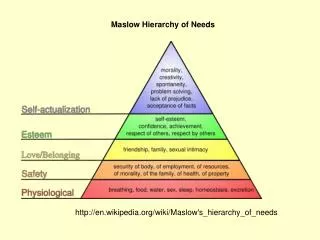
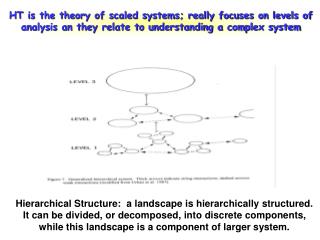
Developing a structure for review Independence Participation Experience Dependence Core Hierachy of Clinical Need
CORE NEEDS FOR EVERY CHILD PAIN FREE COMFORT SECURITY ATTATCHMENT No child can perform at any level of ability unless they have adequate physical and psychological comfort
Pain in the disabled child - problems • Disabled Child – level of Neurological impairment • Anatomy • Physiology • Behavioural • Child - ? Insensitivity pathways • Child - ? Indifference appreciation • Our recognition of their pain • signals • behaviours
Assessment of pain • If able to communicate • Visual analogue scales • Specific communication systems • If unable to actively communicate • Sociability - Crying / ‘distress’ • Facial expression – eyes, brows • Autonomic responses • Motor behaviours – guarding, spasms • Paediatric Pain Profile
Profile- our experience • Facial expression • Change in tone • Protection / Guarding • Autonomic responses - severe discomfort • CARER KNOWS BEST
Where’s the pain coming from ? • 98 children • communicating yet complex physical disability • prospective and retrospective study • one year time span • Results • 86% > 1 episode of significant discomfort over 1 year • 34 % - chronic significant pain ( > 1/52 over 1/12) • symptomatic reflux / spine / hips / spasms
Interventions • HOLISTIC MANAGEMENT • Emotional • Nutritional • Postural • Specifics – Assessment Qualification and quantification Therapy
Botulinum Toxin and Pain management • Hip discomfort – GMFCS 4,5 • Functional difficulties • Posture, Dressing, Toileting, Sleeping • Assess • MDT, paediatric pain service • Intervene • Targeted injections • Re-assess • Keep on top of it
Botulinum Toxin in Hip spasticity • 6months • 27 new children, adolescents in pain • PPP pre average 39 (range 24 – 59) • Functional challenges • Toileting • Cleanliness • Dressing • Sleeping • USS guided injections to • Iliopsoas, Medial Hamstrings, Adductor Magnii
Botulinum Toxin in Hip spasticity • 6 months • 27 new children, adolescents • PPP pre average 39 (range 24 – 59) • PPP 1 month post average 9 (range 0 – 23) • Functional improvements • Toileting • Cleanliness • Dressing • Sleeping
60 Paediatric Pain Profile Scores Pre and Post targeted Botulinum Toxin Injections 50 40 SCORE 30 20 10 PRE 1 MONTH POST
Pain rant summary • Pain in severely disabled children and young people • Under assessed • Under managed • Often only recognised when removed • Holistic management • Botulinum Toxin injections more useful in non-ambulant population • Hip spasm and pain • Sleep, Function and Posture
LEVEL 2 FULL DEPENDENCE • Physically • minimise negative impact of medical disorders seizures / infections • adequate nutrition? • Psychologically • encourage self identity, whilst acknowledging total dependence Basic Clinical …needs met? Psychological Self identity
Nutrition • Key need for development • Primary growth disorders - Neurodisability • Problems • Gastro-Oesophageal Reflux • Absorption • Input : Output • Dribbling
Feeding problems • How much of a problem is it? • Interdisciplinary management • Assessment • Management • Referral pathways
How much of a problem? • Co-ordination of oral-motor function • 81% of children with Cerebral Palsy have some feeding problems (37-98%) • The more severe the motor disorder, the greater the problem
Oral-Motor skills • 6 cranial nerves • Cerebral Cortex and brain stem • Co-ordinate 31pairs of muscles • Oral preparatory • Oral phase • Pharyngeal phase • Oesophageal phase
Co-ordination of swallow • Not helped by difficulties in:- • Postural control • Neurological control - abnormal movements • Vision • Hearing • Communication
Impact of feeding difficulties • Psychological • Child • Family / Carers • Physiological • Growth problems • Bone density • Specific deficits • Health • Reflux / Constipation
Assessment • Interdisciplinary team • Dietary intake • Rate of growth • Assessment of oral motor skills • Medical examination for risk factors • Gastro-oesophageal reflux • Aspiration • Constipation
Management • Posture of feeding • Clinical support • gastro-oesophageal reflux, motility, constipation • Nutritional support • supplements
Referral • At risk • Insufficient intake • Growth failure • Aspiration - frequent chest infections • Gastro-oesphageal reflux • ‘Surgical’ assessment • Investigations • Surgical interventions
Feeding rant summary • Feeding difficulties are common • Careful assessment is needed • Regular monitoring is needed • Interdisciplinary management • Increasing numbers need surgical intervention
Level 3 Experience • Facilitating self control within environments • Home • Play • School Passive and active participation • INPUT • Communication • Movement • Education • Physical needs • Emotional needs Level 4 Choices • Operational level • Change of environment • Allowing the individual child to make choice about their lives Active decision making
Level 5 Independence Can the individual control their environment? If it is possible and appropriate, then the individual should be encouraged to take active control of their own needs
Summary Each child is a dynamic individual(whatever the doctor says) • Their needs and abilities should be regularly re-appraised • They should not be stressed to perform inappropriate tasks • Their physical and psychological core needs of comfort and security should be paramount to all members of their multidisciplinary team