Download
1 / 1
10 likes | 112 Views
The Lowdown on High Doses: Opioid Medications for Chronic Low Back Pain. Joshua Splinter, Tamara Armstrong PsyD , Sandra Burge PhD University of Texas Health Science Center at San Antonio Christus Santa Rosa Family Medicine Residency Program, San Antonio TX. INTRODUCTION. RESULTS.

E N D
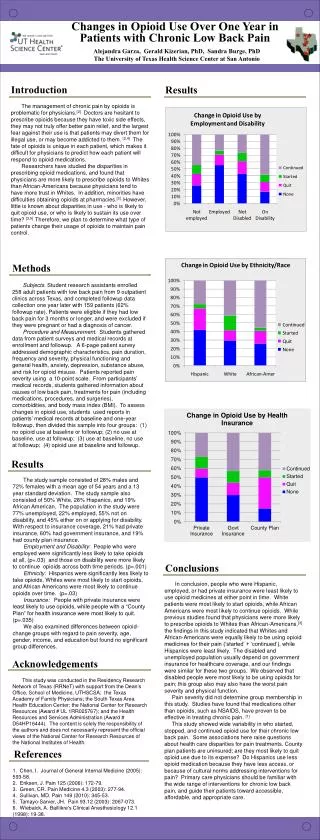
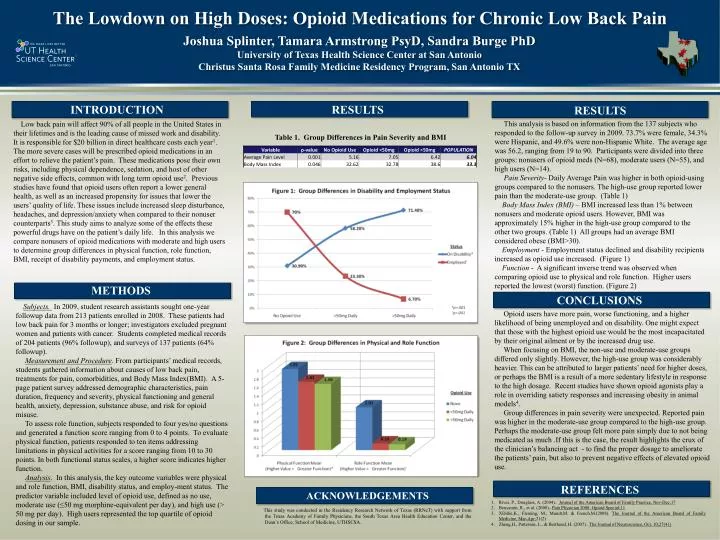
The Lowdown on High Doses: Opioid Medications for Chronic Low Back Pain Joshua Splinter, Tamara Armstrong PsyD, Sandra Burge PhD University of Texas Health Science Center at San Antonio Christus Santa Rosa Family Medicine Residency Program, San Antonio TX INTRODUCTION RESULTS RESULTS This analysis is based on information from the 137 subjects who responded to the follow-up survey in 2009. 73.7% were female, 34.3% were Hispanic, and 49.6% were non-Hispanic White. The average age was 56.2, ranging from 19 to 90. Participants were divided into three groups: nonusers of opioid meds (N=68), moderate users (N=55), and high users (N=14). Pain Severity- Daily Average Pain was higher in both opioid-using groups compared to the nonusers. The high-use group reported lower pain than the moderate-use group.(Table 1) Body Mass Index (BMI) – BMI increased less than 1% between nonusers and moderate opioid users. However, BMI was approximately 15% higher in the high-use group compared to the other two groups. (Table 1) All groups had an average BMI considered obese (BMI>30). Employment - Employment status declined and disability recipients increased as opioid use increased. (Figure 1) Function - A significant inverse trend was observed when comparing opioid use to physical and role function. Higher users reported the lowest (worst) function. (Figure 2) Low back pain will affect 90% of all people in the United States in their lifetimes and is the leading cause of missed work and disability. It is responsible for $20 billion in direct healthcare costs each year1. The more severe cases will be prescribed opioid medications in an effort to relieve the patient’s pain. These medications pose their own risks, including physical dependence, sedation, and host of other negative side effects, common with long term opioid use2. Previous studies have found that opioid users often report a lower general health, as well as an increased propensity for issues that lower the users’ quality of life. These issues include increased sleep disturbance, headaches, and depression/anxiety when compared to their nonuser counterparts3. This study aims to analyze some of the effects these powerful drugs have on the patient’s daily life. In this analysis we compare nonusers of opioid medications with moderate and high users to determine group differences in physical function, role function, BMI, receipt of disability payments, and employment status. Table 1. Group Differences in Pain Severity and BMI METHODS CONCLUSIONS Subjects. In 2009, student research assistants sought one-year followup data from 213 patients enrolled in 2008. These patients had low back pain for 3 months or longer; investigators excluded pregnant women and patients with cancer. Students completed medical records of 204 patients (96% followup), and surveys of 137 patients (64% followup). Measurement and Procedure. From participants’ medical records, students gathered information about causes of low back pain, treatments for pain, comorbidities, and Body Mass Index(BMI). A 5-page patient survey addressed demographic characteristics, pain duration, frequency and severity, physical functioning and general health, anxiety, depression, substance abuse, and risk for opioid misuse. To assess role function, subjects responded to four yes/no questions and generated a function score ranging from 0 to 4 points. To evaluate physical function, patients responded to ten items addressing limitations in physical activities for a score ranging from 10 to 30 points. In both functional status scales, a higher score indicates higher function. Analysis. In this analysis, the key outcome variables were physical and role function, BMI, disability status, and employ-ment status. The predictor variable included level of opioid use, defined as no use, moderate use (≤50 mg morphine-equivalent per day), and high use (> 50 mg per day). High users represented the top quartile of opioid dosing in our sample. Opioid users have more pain, worse functioning, and a higher likelihood of being unemployed and on disability. One might expect that those with the highest opioid use would be the most incapacitated by their original ailment or by the increased drug use. When focusing on BMI, the non-use and moderate-use groups differed only slightly. However, the high-use group was considerably heavier. This can be attributed to larger patients’ need for higher doses, or perhaps the BMI is a result of a more sedentary lifestyle in response to the high dosage. Recent studies have shown opioid agonists play a role in overriding satiety responses and increasing obesity in animal models4. Group differences in pain severity were unexpected. Reported pain was higher in the moderate-use group compared to the high-use group. Perhaps the moderate-use group felt more pain simply due to not being medicated as much .If this is the case, the result highlights the crux of the clinician’s balancing act - to find the proper dosage to ameliorate the patients’ pain, but also to prevent negative effects of elevated opioid use. REFERENCES ACKNOWLEDGEMENTS • Rives, P., Douglass, A. (2004).. Journal of the American Board of Family Practice, Nov-Dec;17 • Benyamin, R., et al. (2008)..Pain Physician 2008: Opioid Special;11 • XDillie,K., Fleming, M., Mundt,M. & French,M.(2008). The Journal of the American Board of Family Medicine, Mar-Apr;21(2) • Zheng,H., Patterson, L., & Berthoud, H. (2007).. The Journal of Neuroscience, Oct. 10;27(41) This study was conducted in the Residency Research Network of Texas (RRNeT) with support from the Texas Academy of Family Physicians, the South Texas Area Health Education Center, and the Dean’s Office, School of Medicine, UTHSCSA.