Download
1 / 48
540 likes | 987 Views
Neuromodulation for Failed Back Surgery Syndrome Part I. Richard K. Osenbach, M.D. Director of Neuroscience and Neurosurgery Cape Fear Valley Health System Fayetteville, NC. Pain Treatment Continuum. Why Neuromodulation?. Testable Completely reversible Non-destructive

E N D
Neuromodulation for Failed Back Surgery SyndromePart I Richard K. Osenbach, M.D. Director of Neuroscience and Neurosurgery Cape Fear Valley Health System Fayetteville, NC
Why Neuromodulation? • Testable • Completely reversible • Non-destructive • No limitation to future therapy
Patient Selection Criteria forImplantable Pain TherapiesSCS and IT Drug Delivery • Failure of more conservative therapies • Further surgical intervention is not indicated • Absence of serious untreated drug habituation • Psychological evaluation and clearance for implantation has been obtained • No contraindications to implantation exist. • sepsis, coagulopathy, etc. • Successful screening trial
Indications for Psychological Consult • Outcome of diagnostic testing, suspected pathology, signs & symptoms do not fit • Markedly unusual reaction either positive or negative to medicine / treatments • Suspicion of emotional “instability” • “Personality” concerns • Suspicion of poor / inadequate / inappropriate coping, fears, beliefs, distress, expectations, and / or attributions
Suggested Referral Questions forPsychological/Behavioral Evaluation • Identify any untreated or under treated major affective disorder • Axis II (personality/character) disorder – Affects if such disorder on the perception of pain, compliance, cooperation, etc. • Any untreated or under treated alcohol or drug problems; present or past • Exceptions/attributions regarding pain and proposed therapy • Nonphysical factors – Their contribution to patient’s pain perception and behavior • Type and degree of social support
Psychological Report • Name:__________________ • Date:___________________ • Diagnosis: Crazy: _____ Not Crazy: _____ Signed: U. R. Nuts, Psychologist
Principles of Screening • Identify and accurately select patients who will achieve long-term success following implantation of a SCS or ITDD system • Goals should be discussed and defined by both the physician and patient BEFORE the trial • Goals are not uniform across patients – they need to be defined on a case-by-case basis • Trial should approximate as closely as possible the conditions of long-term therapy • SCS represents a SINGLE element in overall long-term pain management for a given patient
Assessment of SCS TrialWhat Constitutes Success? • Success of an SCS trial must be defined in the context of the goals that are set prior to the trial • Functional improvement • Mood • Medication use • Analgesic response • What is significant? • “One man’s junk is another man’s treasure”
A SUCCESSFUL TRIAL DOES NOT GUARANTEE LONG-TERM SUCCESS OF A PAIN IMPLANT • 50% OF PATIENTS WHO HAVE IPG FAILURE OR PUMP BATTERY FAILURE NEVER HAVE THEIR DEVICE REVISED
Everything Isn’t A Nail Treating chronic pain is like building a house…..you need more than one tool to successfully build a house. Similarly, chronic pain can not be successfully managed over the long term with a single modality.
SPINAL CORD STIMULATION
History of Spinal Cord StimulationGate Control Theory of Pain Melzack and Wall
History of Spinal Cord StimulationShealy, 1969 • 1967 – Long and Wall, PNS • 1969 – Shealy, SCS in humans • 1975 – Dooley, perc. electrode • Mid 1970s – self-powered battery • 1980s - programmable quad electrode • 1980s -1990s – Primary cell IPG • 2004 – Rechargeable IPG
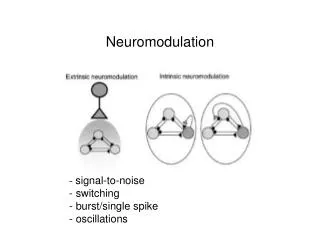
Mechanisms of SCS • Gate control theory • Direct inhibition of spinothalamic neurons • Descending modulatory effects • Alteration of sympathetic activity • Neurochemical modulation
Duration of Screening Trial • Standard of care - trial of at least a couple days duration • No clear data to suggest that trial duration has a significant influence on outcome • Do longer trials confer any advantage? • Allows adjustment of stimulation parameters if needed • Is there a “placebo” effect? • Do positive effects of stimulation persist through the entire duration of the trial? • Assessment of function
Essential Information from Trial • Is there adequate paresthesia overlap of the pain? • Can coverage be obtained with multiple contacts? • Did coverage of different pain areas require different electrode combinations? • Stimulation parameters to achieve the ideal results? • Were there any adverse effects of stimulation? • Painful stimulation, root/trunk stimulation • What degree of analgesia was achieved? • Were the goals of the trial as determined by the patient and physician met?
Screening Methods for SCS Temporary percutaneous trial • Electrode removed at conclusion of trial • Ideal screening method • Lower expectation of success Tunneled percutaneous trial • Electrode intended to be permanent • No considerations for surgical lead • High likelihood trial will be successful • 2nd procedure always required • Higher risk of infection (?) • Ensures reproducible stimulation pattern Surgical lead trial • Inability to place percutaneous leads • Prior spinal decompression • C1-2 electrodes
GOLDEN RULE OF SCS ANALGESIA DEPENDS ON THE PERCEPTION OF STIMULATION-INDUCED PARESTHESIAS THAT OVERLAP THE PAINFUL AREA!!!
SCS – The Biggest Lies Ever Told “Don’t worry, the permanent stimulator will work better than the trial” “This device is going to relieve all of your pain”
Permanent Implant Decision Making • Percutaneous or surgical lead • Complexity of pain pattern • Likelihood of lead migration • Prior spinal surgery • Single or multiple electrodes • Bilateral pain = multiple electrodes • Component of axial pain • Likelihood of pain to change over time • Primary cell vs. rechargeable IPG • Power requirements • Patient convenience and compliance • Cognitive capacity of patient
Percutaneous (Wire) Electrodes • Easy to insert • Ability to “custom design” system • Ideal for screening trial • Avoids 2nd procedure • Subject to migration • Especially in cervical spine • Insertion difficult following posterior decompression • Circumferential contacts • May have higher power requirements
Plate or Surgical Electrodes • Laminotomy required • Less migration and reduced revision rates • Easier to place after laminectomy • Insulated contacts may reduce power requirements • Fixed arrays
Power Sources • External RF system • More power and flexibility • Inconvenience for patient • Unable to use during certain activities • Difficulty in manipulating system • Coupling problem • Primary cell IPG system • More convenient • Finite battery life • Rechargeable IPG system • Extended battery life • 16 contacts – • Increased programming flexibility • Requires recharging by patient
Device Selection Matrix Primary Cell IPG Rechargeable IPG RF System
Anesthesia for SCS Implant • Local anesthesia with IV sedation • Avoid benzodiazepines • Infiltration of periosteum • Injection of local anesthetic epidurally • General anesthesia • Radiological position • Evoked motor responses • C1-2 paddles • Lumbar nerve root • Sacral paddles • Spinal anesthesia • Require less patient sedation • Does not usually influence ability to produce stimulation • Perception thresholds may be slightly higher
Complications of SCS • Bleeding problems • Spinal epidural hematoma • Wound hematoma/seroma • Infection • Wound infection • Spinal epidural abscess • Neurological injury • Lumbar puncture headache • Electrode migration or fracture
Probability of Success • Reflex sympathetic dystrophy • Radicular pain • Brachial plexitis • Peripheral vascular disease • Angina High Low back pain Moderate • Perineal pain • Rectal pain • Zoster pain • Anesthesia dolorosa Low
? ? ? Radiculitis Persistent Pain in a Radicular Distribution That Does Not Respond To Conventional Treatment
T10-S1 Fusion for L3 Neuropathic Pain !!!!! In a 70 Y/O Woman no less!!!
The Low Back • So what about getting the low back? • Several hypothetical reasons for why it is a challenging target • Sensory homunculus • Small body area relative to legs • Probably evenly distributed in DC
L2-L5 Dermatomes • If the ‘receptive fields’ per nerve are equal, then there would be at least 4 times fewer fibers for back coverage than leg coverage 80% 20%
Anterior leg fiber Low Back Fiber Fiber Distribution within Dorsal Columns DC fibers of L2 Dermatome • Finally, within the “slice” of DC that our L2 dermatome represents, it makes sense to think that leg fibers and back fibers would be evenly spread out in the slice • In other words, a low back fiber is just as likely to be on top of the DC’s as at the bottom
Sacral Fibers Lumbar Fibers Thoracic Fibers Anterior leg fiber Low Back Fiber What Does All of This Mean DC fibers of L2 Dermatome • So, Low Back fibers aren’t especially important from a functional standpoint • Few… • And Low Back fibers don’t cover much body surface area (relative to legs, with which they share dermatomes) • Fewer… • And Low Back fibers aren’t especially “available” for stimulation in the DC’s • May be hard to reach enough of them to get good coverage
Target: Usually Dorsal Columns. Why? Minimal Side-Effects: DC has primarily sensory fibers – if you activate them, the patient will pretty much only get sensation, not motor or autonomic effects Efficient: DC is very “rich” – all the body parts/dermatomes below the level of the lead may be stimulated from that lead position Example: sometimes if you stimulate in the cervical region, you can get whole body paresthesia. To avoid (generally): Dorsal Roots. Why? Side-Effects: DR’s carry all sorts of sensory fibers, not just touch and vibration, but also pain and motor reflex. If you maximize DR stimulation, the patient might start feeling sharp pain or actually get muscle contractions Inefficient/Inadequate: DR’s will only generate paresthesia in a few dermatomes, those represented at that spinal level Example: if the lead is at T9, and you stimulate the DR fibers there, the patient will report a “narrow band” of paresthesia in the chest wall. What Do We Want to Stimulate and Where Should We Place the Lead???
General Principles of Lead Postioning • Clinically, the most effective stimulation is elicited from electrodes placed within 3mm of midline • Axial structures best stimulated with midline electrodes • Upper extremity stimulated relatively easily with either midline or laterally-placed electrodes • Chest/abdomen best stimulated with more laterally-placed electrodes • Lower thoracic region – lateral electrodes more common stimulate anterior part of leg; posterior leg more easily stimulated from midline • Avoid overdriving one area to achieve stimulation in another
Electrical Field Shaping Dual Lead Bipole Single Lead Bipole Single Lead Guarded Array Transverse Guarded Array
Pitfalls of Spinal Cord Stimulation • Lack of patience (not patients) during intraoperative screening • Trial too short in duration – placebo effect • “False negative” trial • Use of different electrode configurations from screening to permanent implant
Brachial Plexus Stretch Injury C2-3 C7-T1 Electrode Location Pain in the jaw, neck, upper extremity Pain in the axilla, upper chest wall and C8-T1 distribution
SCS vs. Reoperation vs. DRG Dorsal RootGanglionectomy Reoperation Spinal Cord Stimulation Percent of Patients* * Patients reporting pain relief in excess of 50% North et al., Neurosurgery, 1991
Reduction in Pain 50% - 60% of patients will derive at least 50% reduction in pain with spinal cord stimulation
Return to Work 2% 19% Length of Time Off Work 94% Percentage Who Return to Work J. McGill, J Occupational Medicine, 1968
Cost Benefit Analysis of Neurostimulation Mekhail et. al., Clin J Pain, 2004:462-468 • Assessment of healthcare utilization prior to SCS implantation • Net differences in events per year calculated and modeled to 2000 cost data from CMS Fee Schedule and Healthcare Financing Administration • Net annual savings of $30,221; $93,685 over 3 year implant duration • $17,903 net per patient per year cost savings • Reduction in physician office visits, ER visits, imaging procedure, nerve blocks, hospitalizations, and surgical procedures
SCS Cost Benefit Analysis CONCLUSION: Despite the high cost of SCS, there may be substantial long-term economic benefit based on the fact the patient treated with neurostimulaion is more likely to consume healthcare resources at a significantly reduced rate.