Download
1 / 16
160 likes | 279 Views
Best Practice for the MDTM Process. Lal Senaratne MS, FRCS, D.Phil (Oxon) Consultant Vascular Surgeon East Kent Hospitals University NHS Foundation Trust. What I will do. Describe what we do in Kent Raise some issues Conclude Re:Best Practice. Our patch. Medway. Canterbury.

E N D
Best Practice for the MDTM Process Lal Senaratne MS, FRCS, D.Phil (Oxon) Consultant Vascular Surgeon East Kent Hospitals University NHS Foundation Trust
What I will do . . . • Describe what we do in Kent • Raise some issues • Conclude Re:Best Practice
Our patch . . . Medway Canterbury
What we have . . . • 2 Centres • Network solution • Joint MDTM for AAAs
Who is in our MDTM . . . • Vascular Surgeons • Interventional Radiologists • Vascular Anaesthetists • Junior doctors/trainees • Vascular Nurse practinoners • Secretary • Others
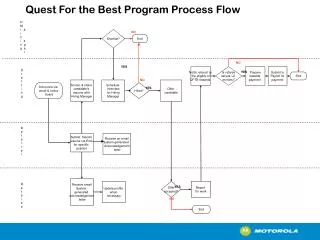
Our MDTM process Reaching threshold in surveillance programme Incidental finding Screen detected Asymptomatic Aneurysms Symptomatic Aneurysms Discussions outside MDTM Pre-op Ix MDTM Discussion Written communication to Pt & GP Anaesthetic Review Out pt review Decision to intervene Intervention Open EVAR
What happens at our MDTM … • Play video clip
Issues . . . • When there is no consensus • When Ix not ready • Should symptomatic aneurysms be included? • Does it introduce delay? • Documentation issues • Time wasting! (Needless/endless discussion)
Best Practice • Right Team • Right information • Right patient • Consensus as far as possible • Tertiary opinion Right decision
Thank you Any questions?