Download
1 / 19
190 likes | 382 Views
Walking. Wael Alasaq PT. Ph.D. Kuwait University PT Dep. 1.1-1.5 m/s community functional speed. Only 7% of discharged pts are able to walk 500 m continuously @ a safe speed (Rd X). Walking requires. Ability stand up against gravity Move COG Maintain COG within BOS.

E N D
Walking Wael Alasaq PT. Ph.D. Kuwait University PT Dep.
1.1-1.5 m/s community functional speed. • Only 7% of discharged pts are able to walk 500 m continuously @ a safe speed (Rd X)
Walking requires • Ability stand up against gravity • Move COG • Maintain COG within BOS
Walking dysfunction is very common in pt with stroke. • Mainly due: - Muscle weakness & paralysis - Poor motor control - Soft tissue contractures - Adaptation (as he/she tries to walk despite the problems present)
Requirement for successful walking • Stability (support by the LL) & dynamic balance • Progression requirement (propulsion of the body in the desired/intended direction) • Basic locomotor rhythm • Adaptation requirement ( to changing environment)
Gait cycle • Two phases stance & swing • Stance apprx 60% of the gait cycle • Wt acceptance • Med stance • Push off • Swing apprx 40% of gait cycle • Early swing • Late swing
Gait cycle cont In some texts the phases are divided to more subphases. Stance to five: • Initial contact • Loading response • Mid-stance • Terminal stance • Pre-swing
Gait cycle cont Swing phase subdivided to 3: • Initial swing • Mid-swing • Terminal swing
Gait cycle cont. • @ end of each phase & beginning of the other there are periods of double support (80% of the cycle)
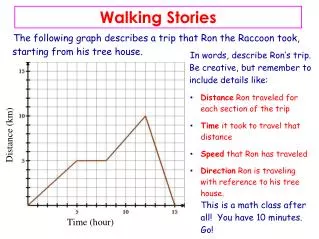
Spatiotemporal Variables of gait • Cadence • Stride length • Step length • Velocity • # of steps per min • The distance covered from one heel strike to the following heel strike, by the same foot. • Distance from on foot strike to the foot strike of the other foot. • The average horizontal speed of the body measured over one or more strides
Muscle activity The main role is to provide the mechanical power for • Keeping the body in the upright position, ie support against gravity, • Moving body segments, mainly around three major joints What are they?
Age related changes • Slower walking speed • Stride length decrease • Increase in duration of double support • Decrease in vision • Decrease in cardiovascular capacity • Muscle strength • Joint flexibility • Bone mass
Variability in gait following stroke • Mainly due: - Muscle weakness & paralysis - Poor motor control - Soft tissue contractures - Adaptation (as he/she tries to walk despite the problems present)
Variability in gait following stroke Cont. In stroke pt , Research have found • Decrease in hip extension @ end of stance • Decrease in hip flexion in mid swing • Decrease in knee flexion @ toe-off & mid- swing • Decreased dorsiflexion @ foot contact, & during stance associated with hyperextended knee. • Decreased ankle plantarflextion @ toe-off • Increased knee flexion @ foot contact.
Please refer to your book for understanding the difference between the Typical & atypical kinematics of the gait. • Tip: Make a table of comparison for ease reference.
Guidelines for training Aims of intervention is optimization of walking performance by: • Preventing adaptive changes in LL soft tissues. • Eliciting voluntary contraction in key mm grp in LL. • Increase muscle strength & coordination
optimization of walking performance cont. 4. Increase walking velocity & endurance. 5. Maximize skill, ie increasing flexibility. 6. Increasing cardiovascular fitness.
Practice in groups Using your book start from p 100