Download
1 / 83
840 likes | 1.22k Views
Inflammatory Disorders of Larynx. Dr. Vishal Sharma. Classification. A. Acute infection B. Chronic infection Acute s imple laryngitis Chronic laryngitis Acute epiglottitis Tuberculosis Viral LTB Scleroma Bacterial LTB Candidiasis

E N D
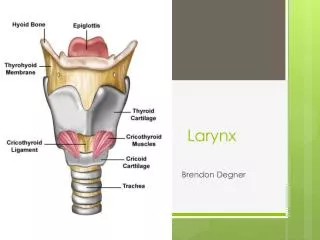
Inflammatory Disorders of Larynx Dr. Vishal Sharma
Classification A. Acute infection B. Chronic infection Acute simple laryngitis Chronic laryngitis Acute epiglottitis Tuberculosis Viral LTB Scleroma Bacterial LTB Candidiasis Spasmodic croup Sarcoidosis C. Laryngeal edema D. Laryngo-pharyngeal reflux disease (LPRD)
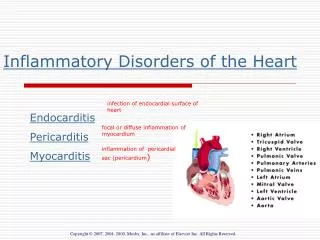
Causes for laryngeal edema Laryngeal infections Retropharyngeal abscess / quinsy / Ludwig’s angina Angio-neurotic edema; Reinke’s edema Thermal / caustic burn Trauma: accidental / intubation / endoscopy Ca of larynx / pharynx; Post-irradiation Nephritis / heart failure / myxedema / anasarca
Etiology • Viral infection (common cold) • Vocal abuse • Allergy / smoking / environmental pollution • Gastro esophageal reflux disease • Thermal / chemical burn due to inhalation • Use of asthma inhalers • Laryngeal trauma (endotracheal intubation) • Undue physical or psychological stress
Clinical Features • History of upper respiratory tract infection • Hoarseness: high pitched husky voice • Dry, paroxysmal cough, mainly at night • Sore throat worsened by talking; fever, malaise • Laryngoscopy:red, swollen supraglottic mucosa; mild erythema / swelling of true vocal cords; inspissated secretions b/w vocal cords
Treatment • Prevention: avoidance of cold fluids, cold air, smoking, alcohol consumption • Absolute voice rest • Tincture Benzoin steam inhalation & mucolytics • Anti-tussives: dextromethorphan, codeine • Pantoprazole for GERD; analgesics for pain • Antibiotics: for secondary bacterial infections • Steroid:for laryngeal edema
Synonym:Acute Supraglottitis Supraglottic laryngitis Definition:Rapidly developing inflammation of epiglottis & adjacent tissues, due to bacterial infection, may cause life-threatening airway obstruction Causative agents:Haemophilus influenzae type b (Hib), Streptococcus pyogenes, Streptococcus pneumoniae, Staphylococcus aureus
Symptoms • Distress (respiratory) • Dysphagia • Drooling (due to inability to swallow) • Severe sore throat / odynophagia • Muffled voice • Sudden onset & rapid progression in children (in hours); Indolent course in adults (in days)
Examination • Simply depressing child's tongue with tongue depressor or indirect laryngoscopy may visualize enlarged, cherry red epiglottis in some situations • These procedures may precipitate complete airway obstruction, hence avoided
Tripod sign • Pt appears anxious • Leans forward with support of both forearms • Extends neck in an attempt to maintain an open airway
Investigations 1. Flexible laryngoscopy:carried out only in ICU or OT with intubation / tracheostomy set ready 2. Post-intubation direct laryngoscopy 3. Plain x-ray soft tissue of neck lateral view 4. Culture from epiglottis during intubation:+ve in 15% cases of H. influenzae 5. Blood culture:+ve in 15% cases of H. influenzae
Flexible laryngoscopy • Inflamed cherry-red epiglottis • Thickened aryepiglottic folds • Edematous arytenoid cartilages
X-ray soft tissue neck Lateral view taken in erect position only • Enlargement of epiglottis (thumb sign) • Absence of well defined vallecula (Vallecula sign) • Thickening of aryepiglottic folds (cause for stridor) • Circumferential narrowing of subglottic portion of trachea during inspiration (25% cases) • Ballooning of hypopharynx
X-ray soft tissue neck • Red arrow = enlarged epiglottis • Yellow arrow = thickened ary-epiglottic folds
Treatment • Hospitalization, careful monitoring & isolation • Hydration + humidification + oxygen tent therapy • Secure airway in acute stridor → Mechanical ventilation till swelling + inflammation subside • IV Ceftriaxone: 100 mg/kg/d in 2 divided doses • Hydrocortisone: 100 mg IV stat & 25 mg Q8H • Rifampicin prophylaxis for household contacts
Methods of securing airway • Endotracheal intubation • Trans-nasal: preferred • Trans-oral • Percutaneous trans-laryngeal ventilation by needle cricothyrotomy • Tracheostomy: last resort for acute stridor
Prevention • Hib vaccination for all children • Rifampicin prophylaxis (20 mg/kg /day; max. 600 mg) for 4 days should be given to all household contacts if: a. child in household < 4 years, not received appropriate doses of Hib vaccine b. immuno-compromised child, despite vaccination • Children > 2 years with epiglottitis do not need vaccination as disease provides immune protection
Acute viral LTB (Croup) • Commonest infective cause of stridor in children • Mean age for presentation = 18 months • Causative agents: • Parainfluenza virus type I, II, III • Influenza virus • Respiratory syncytial virus • Rhinovirus • Measles
Clinical Features • Gradual onset preceeded by URTI of > 48 hrs • Hoarseness • Biphasic stridor, mainly at night • Dry cough (like barking of seal) • Low grade fever (< 102 F) • Child prefers to lie down, but is restless • Dysphagia & drooling absent
Investigations • Plain X-ray soft tissue neck, AP view a. Church steeple or pencil-point sign: squared appearance of subglottic area replaced by cone shaped narrowing just below vocal cords b. Ballooning of hypopharynx • Flexible laryngoscopy:narrowed subglottic area
Treatment • Hospitalization • Humidification & mucolytic drugs • Hydration with IV fluid • Hydrocortisone: 100 mg IV stat & 25 mg Q8H • Oxygen tent:es bronchospasm & pulm. edema • Antibiotic (IV Ceftriaxone): 100 mg/kg/day • Racemic adrenaline (1:1000) nebulization • Intubation / Tracheostomy for acute stridor
Bacterial LTB Synonym:pseudo-membranous croup More severe than viral LTB Causative agent: Staphylococcus aureus Pathology: sloughing of respiratory epithelium C/F:Hoarseness, biphasic stridor, dry cough, high grade fever (> 102F), child supine but restless X-ray neck, AP view: church steeple sign Rx:moist air + oxygen + antibiotics
Subglottic laryngitis • Synonym:spasmodic croup • Etiology:unknown (? Influenza virus infection) causing subglottic mucosal edema • C/F:Child below 3 years with rapid onset of biphasic stridor + barking cough + low grade fever (< 102 F). Dysphagia & drooling are absent. • X-ray neck, AP view:church steeple sign • Rx:Moist air + oxygen + supportive treatment. Rarely endotracheal intubation. Avoid sedatives.
Definition:Chronic non-specific inflammation causing irreversible changes of laryngeal mucosa Etiology of chronic laryngitis: • Viral infection (common cold) • Vocal abuse • Allergy / smoking / environmental pollution • Gastro esophageal reflux disease • Thermal / chemical burn due to inhalation • Laryngeal trauma (endotracheal intubation) • Undue physical or psychological stress
Chronic hyperemic laryngitis Hoarseness (worse in morning) + dry cough for > 3 wk Persistent clearing of throat H/o previous URTI / GERD may be present Laryngoscopy:hyperemic laryngeal mucosa with sub-mucosal edema Treatment:Voice test + medicated steam inhalation + systemic antibiotic. Avoidance of alcohol & tobacco. Reversible within few weeks.
Chronic hyperplastic laryngitis Hoarseness (worse in morning) + dry cough for > 3 wk Persistent clearing of throat H/o previous URTI / GERD may be present Laryngoscopy: • Mild congestion of laryngeal mucosa • Patches of epithelial thickening • Broad based polypoid lesions
Chronic laryngitis histology Kleinsasser’s classification: • Grade I:simple squamous cell hyperplasia or keratosis • Grade II:squamous cell hyperplasia + atypia (mild to moderate dysplasia) • Grade III:carcinoma in situ with intact basal membrane
Rx of hyperplastic laryngitis Absolute voice rest for 48 hours Systemic antibiotic Tincture Benzoin steam inhalation Analgesics & anti histamine-decongestant Micro-laryngoscopic excision of lesion & HPE • Grades I & II: no further treatment • Grade III: total excision of lesion / radiotherapy
Prevention of recurrent attacks • Avoid breathing polluted air • Avoid tobacco in any form (chewing, smoking) • Avoid recreational drugs like marijuana • Avoid alcohol consumption • Avoid talking or shouting at noisy places • Avoid continuous throat clearing • Avoid whispering loudly
Introduction Accumulation of fluid in Reinke’s space Synonyms:Bilateral diffuse polyposis, Smoker’s polyps, Polypoid corditis, Polypoid degeneration of vocal cords, Localized hypertrophic laryngitis 10% of benign laryngeal lesions