Download
1 / 85
850 likes | 1.23k Views
Clinical Protocol Writing 101 Massachusetts Biotechnology Council 6 March 2009 Michelle Currie Vice President, Clinical Operations, Veristat, Inc. Christopher Schoonmaker, MPH Associate Director, Biostatistics, Veristat, Inc. Presentation summary. Definition of a protocol

E N D
Clinical Protocol Writing 101 Massachusetts Biotechnology Council 6 March 2009 Michelle Currie Vice President, Clinical Operations, Veristat, Inc. Christopher Schoonmaker, MPH Associate Director, Biostatistics, Veristat, Inc.
Presentation summary • Definition of a protocol • Developing a study-specific protocol, including statistical methodology • Protocol amendments • Protocol template format / content • The protocol and CDISC
What is a protocol The International Conference on Harmonisation (ICH) defines a protocol as follows: “A document that describes the objective(s), design, methodology, statistical considerations, and organization of a trial. The protocol usually also gives the background and rationale for the trial, but these could be provided in other protocol-referenced documents.”
What is a protocol Purposes: • Describes how to treat and manage patients • Describes data to be collected and collection methods • Describes the plan for data analysis • Used to select study centers / vendors • Used by IRBs/IECs to determine whether to approve study • Reference tool for monitoring and auditing study conduct
Questions to consider • What is the study phase? • Phase 1: small sample size; evaluate safety; determine a safe dosage range; identify side effects; ADME • Phase 2: larger sample size; evaluate efficacy and further evaluate safety
Questions to consider • What is the study phase? • Phase 3: large sample size; confirm efficacy, compare to commonly used treatments, and collect data to allow the drug to be used safely • Phase 4: post-marketing; further determine drug's risks, benefits, and optimal use
Questions to consider • What type of study is it? • Treatment study: test experimental treatments, new combinations of drugs, or new therapeutic approaches • Prevention study: ways to prevent disease in naïve subjects or to prevent a disease from returning
Questions to consider • What type of study is it? • Diagnostic study: better tests or procedures for diagnosing a particular disease or condition • Screening study: best way to detect certain diseases or health conditions • Quality of Life / Supportive care study: explore ways to improve comfort and the quality of life for individuals with a chronic illness
Questions to consider • What is the study drug? • What is the indication? • What is the scientific question that needs to be answered (i.e., what are your objectives)? • What is the regulatory question that needs to be answered? • What is the budget?
Questions to consider • Efficacy evaluations: • What tests are appropriate for the indication? • What tests are appropriate for the study drug? • Is a central / independent read of test results needed? • Is a Clinical Endpoint Committee (CEC), or equivalent, necessary?
Questions to consider • Safety evaluations: • How will adverse events be collected? • Are there specific events to be solicited? • What tests are appropriate for the indication? • What tests are appropriate for the study drug? • Is a central / independent read of test results needed? • Is a DSMB or formalized interim review of safety data necessary?
Questions to consider • Ultimately, what do you want to say in the clinical study report (CSR)? • Collect what you need. • Don’t necessarily collect everything everybody wants.
Considerations for patients/participants • Is the visit schedule reasonable / feasible? • Are there invasive / painful study procedures? • How much blood will be collected? • What other samples will be collected (tissue, bone marrow, spinal fluid)?
Considerations for patients/participants • How long will the patient have to stay at the study center? • Are there costs associated with participation? • Are there dietary / life-style restrictions? • Will the patient need access to equipment?
Considerations for study personnel • Is the visit schedule reasonable / feasible? • Are early morning, late evening, or weekend appointments required? • How much data are to be collected? • Are turn-around times required by the protocol feasible per the facilities standard operating procedures?
Considerations for the investigator • Does the investigator have access to patients meeting the eligibility criteria? • Are the eligibility criteria consistent with clinical status of patients? • Is there a reasonable possibility of benefit to patients?
Considerations for the investigator • Are the risks to patients too high? • Does the protocol provide a reasonable treatment option relative to standard of care? • Will patients be subjected to procedures / treatments they don’t need or restricted from procedures / treatments they do need?
Considerations for the sponsor • All of the previous, plus: • How many patients are required? • Are the eligibility criteria reasonable for adequate enrollment? • How many study centers will be required to reach the intended number of patients?
Considerations for the sponsor • Are data needed by a particular date to plan future studies or meet a regulatory requirement? • What is the per-patient cost? • The more frequent the visits, the higher the per-patient cost • The more clinical tests (MRI, CT, X-rays), the higher the per-patient cost
Resources Solicit input from: • Medical monitor • Safety officer • Regulatory representative • Statistician • Drug supply • Clinical data management • Pharmacologist • Commercialization team (marketing, sales)
Reference materials Refer to: • Previous protocols for the study drug/device or for a similar indication • Clinical development plan • Investigator’s brochure • Publications • Internet (e.g., http://clinicaltrials.gov) • Regulatory guidance documents (general and drug class- or indication-specific)
Reference materials Do not feel compelled to rewrite what has already been written (provided it is well-written) • If it ain’t broke, don’t fix it
Protocol concept Development of protocol concept “sheet” recommended (but not required). • Protocol concept essentially is the protocol synopsis • Focuses on key details • Limits the need to revise text across multiple sections • Review and approve before developing full protocol
Protocol concept Generally contains: • Protocol Title • Protocol Number • Study Phase • Investigators and Study Centers • Objectives • Study Design • Number of Patients Planned
Protocol concept • Diagnosis and Main Criteria for Inclusion • Test Products, Doses, and Administration Mode • Duration of Treatment • Study Endpoints: • Efficacy • Pharmacokinetic / pharmacodynamic • Safety • Statistical Methods • Evaluation Schedule
Protocol concept First Steps • Determine: • Objectives / Endpoints • Evaluation Schedule, including dose schedule • Sample Size • Eligibility Criteria Other elements of the protocol can be built from these pieces
Diagrams and flowcharts A clear evaluation schedule is critical • Clearly identify study periods / visits • Organize procedures in the order in which they are to be performed • Structure in a way to minimize footnotes
Diagrams and flowcharts Carefully consider the timing of evaluations. For example:
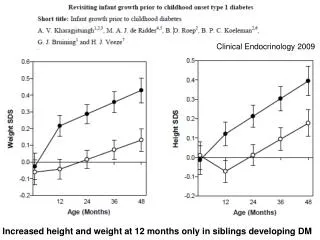
Diagrams and flowcharts Mean (SD) Corrected Calcium (mmol/L) Over Time
Diagrams and flowcharts Mean (SD) Corrected Calcium (mmol/L) Over Time
Diagrams and flowcharts The evaluation schedule is useful for: • Scheduling patient visits • Determining blood collection volumes • Scoping study costs • CRF development
Diagrams and flowcharts • Use other diagrams and charts to illustrate complicated processes and / or reduce text • Consider whether useful to study center personnel
Sample size / power calculation Why is it important? • Will your study be powered to detect statistical significance if one really exists? • Not always necessary for Phase I studies (e.g., dose escalation trials), • Most important for pivotal Phase III and Phase II studies
Sample size / power calculation Why is it important? • As sample size increases, power increases. The higher the power, the lower the type II error • We limit the type II error by powering the study at a high level (generally >= 80%) • We limit the type I error by predefining a low alpha level (generally .05)
Sample size / power calculation What is needed to perform or describe sample size calculations? • Indication of the primary endpoint (e.g., overall survival, disease response) • What is your hypothesis? • What is it that you expect your drug or device to do?
Sample size / power calculation What is needed to perform or describe sample size calculations? • Proposed design(s) of study and phase? • Dose escalation, Simon 2 Stage, randomized control trial, non-inferiority, etc.? • Indication of the number of planned treatment arms
Sample size / power calculation What is needed to perform or describe sample size calculations? • Alpha level for primary and secondary endpoints • Any limitations to the number of subjects you can enroll? • Some statistical methods/tests might be more robust with smaller sample sizes while still maintaining the necessary statistical power. • Estimate of effect size/hypothesized treatment effect/benchmark of treatment success • e.g., estimated median survival of 15 weeks in Arm A versus 20 weeks in Arm B
Description of the planned statistical methods What is needed to write this section? • Assessment schedule (particularly in table form) • A list of all endpoints to be measured • A concept of the critical or important safety evaluations that are needed for the study A protocol concept sheet / synopsis is ideal • Provides description of variables to be collected and when
Description of the planned statistical methods Baseline Evaluations • A brief description of the baseline evaluations and intended variables to be summarized. • For example: “Demographic and baseline disease characteristic data summarization will be performed in order to descriptively assess the comparability of dose groups. Data to be tabulated will include sex, age, and race, as well as disease-specific information.”
Description of the planned statistical methods Safety Assessments • A description of the primary and secondary safety endpoints • Summary of any relevant statistical hypothesis testing including alpha level and/or confidence interval calculations
Description of the planned statistical methods Safety Assessments • Summary of planned analysis for: • adverse events (tabulation of incidence rates) • study drug exposure (cumulative dose received, cycles received, etc.) • laboratory assessments, vital signs, and ECG Analysis (change from baseline, shift tables, etc.)
Description of the planned statistical methods Efficacy Assessments • A description of the primary and secondary efficacy endpoints and intended analysis of each • The planned analysis for the primary endpoint should be very detailed/analysis plan ready, particularly in Phase III • Description of any relevant statistical hypothesis testing including alpha level and/or confidence interval calculations