Download
1 / 61
660 likes | 727 Views
PERIODONTAL PLASTIC AND ESTHETIC SURGERY. Definition. Periodontal Plastic Surgery is defined as the procedures performed to correct the anatomical, developmental and traumatic deformities of gingiva and alveolar mucosa. Terminology .

E N D
Definition Periodontal Plastic Surgery is defined as the procedures performed to correct the anatomical, developmental and traumatic deformities of gingiva and alveolar mucosa.
Terminology • Periodontal Plastic Surgery was previously termed as Muco-Gingival surgery • The term Periodontal Plastic Surgery was originally introduced by Miller in 1993. • AAP world workshop 1996 renamed Muco Gingival Surgery as Periodontal Plastic Surgery.
Objectives • To correct the problems associated with inadequate attached gingiva. • To correct the problems associated with shallow vestibule. • To correct the problems associated with high frenum attachment.
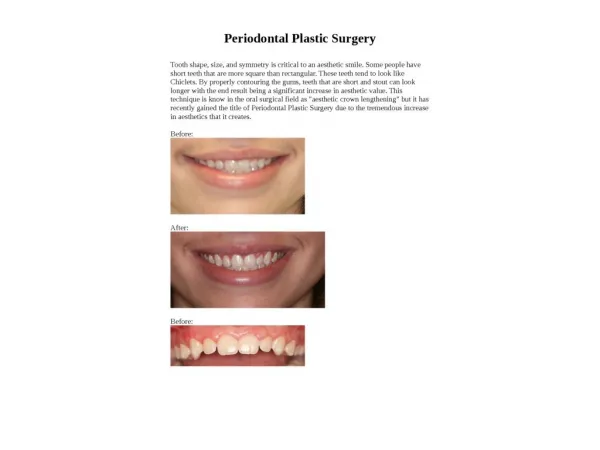
Indications of periodontal plastic surgery • Periodontal prosthetic surgery • Crown lengthening surgery • Ridge augmentation surgery • Esthetic surgical correction. • Coverage of denuded root surface • Reconstruction of papilla. • Esthetic surgical correction around implants
Rationale • Rationale of periodontal plastic surgery was previously predicated on the assumption that a minimum width of attached gingiva is essential to maintain optimum gingival health.
PROBLEMS ASSOCIATED WITH INADEQUATE WIDTH OF ATTACHED GINGIVA
Problems Associated With Inadequate Width of Attached Gingiva • Difficulty in maintaining Optimum Gingival Health. • Improper plaque control. • Difficulty in maintaining Optimum Gingival Health around abutment teeth. • Inadequate keratinized tissue for placement of RPD.
Measurement of Width of Attached Gingiva Width of attached gingiva can be measured by subtracting pocket depth from the distance between free gingival margin to the mucogingival junction.
Measurement of Width of Attached Gingiva and Keratinized Gingiva
Advantages of Creating Adequate Width of Attached Gingiva • Proper plaque removal. • Improved esthetics. • Reduces inflammation around restored teeth.
Techniques For Increasing Width of Attached Gingiva • Free gingival autograft, • Free connective tissue autograft, • Apically positioned flap, • Pedicle autograft, • Subepithelial connective tissue autograft.
Problems Associated With Shallow Vestibule • Improper plaque removal, • Difficulty in placement of removable prosthesis.
SHALLOW VESTIBULE NORMAL VESTIBULARDEPTH
Measurement of Vestibular Depth Depth of vestibule is measured from gingival margin to the bottom of the vestibule.
Advantages of Creating Adequate Vestibular Depth • Proper plaque control. • Proper tooth brushing. • Proper placement of removable prosthesis.
TECHNIQUES • VESTIBULAR DEEPENING (EDLAN- MEJCHAR’S) • FENESTRATION OPERATION • FREE SOFT TISSUE AUTOGRAFT
PROBLEMS ASSOCIATED WITH HIGH FRENUM • IMPROPER PLAQUE REMOVAL • TENSION ON THE FRENUM MAY TEND TO OPEN THE SULCUS
NORMAL FRENUM ATTACHMENT HIGH FRENUM ATTACHMENT
EXAMINATION OF HIGH FRENUM • TENSION TEST IS PERFORMED BY PULLING THE LIPS : IN CASES OF HIGH FRENUM, THERE IS BLANCHING OF THE GINGIVA AND MOVEMENT OF GINGIVAL MARGIN ALONG WITH THE MOVEMENT OF CHEEKS AND THE LIPS
ADVANTAGES OF CORRECTING HIGH FRENUM ATTACHMENT • Proper plaque control. • Reduces inflammation of the gingiva around teeth. • Reduces progression of periodontal disease
TECHNIQUES • FRENOTOMY • FRENECTOMY
GINGIVAL RECESSION • DEFINITION: • EXPOSURE OF THE TOOTH BY THE APICAL MIGRATION OF THE GINGIVA • EXPOSURE OF THE ROOT SURFACE BY AN APICAL SHIFT IN THE POSITION OF THE GINGIVA
GINGIVAL RECESSION IN RELATION TO MANDIBULAR CENTRAL INCISOR NO GINGIVAL RECESSION
ETIOLOGY • FAULTY TOOTH BRUSHING( GINGIVAL ABRASION) • TOOTH MALPOSITIONING. • FRICTION FROM SOFT TISSUE (GINGIVAL ABLATION) • GINGIVAL INFLAMMATION • HIGH FRENUM ATTACHMENT
CLASSIFICATION OF GINGIVAL RECESSION SULLIVAN AND ATKIN’S • SHALLOW –NARROW • SHALLOW –WIDE • DEEP- NARROW • DEEP- WIDE
TECHNIQUES TO MANAGE GINGIVAL RECESSION • FREE GINGIVAL AUTOGRAFT • PEDICLE AUTOGRAFT • FREE CONNECTIVE TISSUE AUTOGRAFT • SUBEPITHELIAL CONNECTIVE TISSUE AUTOGRAFT • GUIDED TISSUE REGENERATION
Miller Class I Recession • Class I • Marginal tissue recession which does not extend to the mucogingival junction • No periodontal bone loss in the interdental area • 100% root coverage
Millers Class II Recession • Class II • Marginal tissue recession which extends to or beyond the mucogingival junction • No periodontal loss in the interdental area • 100% root coverage
Millers Class III Recession • Marginal tissue recession which extends to or beyond the mucogingival junction • Bone or soft tissue loss in the interdental area or malpositioning of the teeth, preventing • 100% root coverage • Partial root coverage
Millers Class IV Recession • Class IV Marginal tissue recession which extends to or beyond the mucogingival junction Severe bone or soft tissue loss in the interdental area and/or malpositioning of teeth No root coverage
Root Coverage Using FreeAutogenous Gingival Grafts Indications All cases where root coverage is necessary except when a graft of sufficient thickness (1.5-2.0 mm) cannot be harvested Contraindications Extensive gingival recession Esthetic cases
Root Coverage Using FreeAutogenous Gingival Grafts • Disadvantages Poor ability to provide blood supply to the graft for root coverage Exposed deep and large wound on the palatal mucosa Inferior esthetic results due to scarring Surgery required in 2 areas
Root Coverage & Increase In Attached Gingiva Postoperatively