Download
1 / 9
110 likes | 330 Views
Referral Management. Review by the Kings Fund 2010. RMCs act as a conduit for all referrals and conduct triage that may redirect or reject referrals. GPs are given clinical guidelines intended to influence their referral behaviour. The referral management spectrum.

E N D
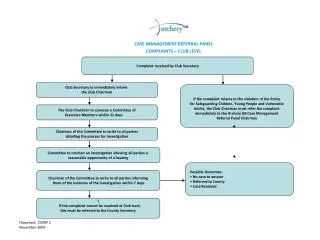
Referral Management Review by the Kings Fund 2010
RMCs act as a conduit for all referrals and conduct triage that may redirect or reject referrals GPs are given clinical guidelines intended to influence their referral behaviour The referral management spectrum
The available evidence suggests… • Not all referrals are clinically necessary, substantial element is “discretionary and avoidable” • Some patients need a referral but don’t get one • A large number of patients seen in secondary care could be seen in another setting • Many referral letters lack the necessary information • There is frequently a “lack of shared understanding” of the purpose of the referral between GP, patient and consultant • Appropriate pre-referral management is often lacking
Purpose of King’s Fund Review • Can referral management effectively control demand and reduce unnecessary referrals? • Can referral management influence other aspects of referral – destination and process? • Can referral management deliver savings? • What are the other risks and consequences of introducing referral management, and how might these be overcome?
KFR 2010: Overview • Nationally, GP referrals to outpatients increased by 19 per cent between 2005 and 2009, • Consultant-to-consultant and other sources of outpatient referral increased at double this rate, 39 per cent and 41 per cent respectively. • Although 50% of PCTs studied believed that their referral management schemes had managed to curtail demand, the evidence suggests that PCTs with active referral management were, in fact, no more likely to curtail demand than were other PCTs.
King’s Fund Review: Conclusions and Recommendations • “A referral management strategy built around peer review and audit, supported by consultant feedback, with clear referral criteria and evidence-based guidelines is most likely to be both cost and clinically effective.” • The greater the degree of intervention, the greater the likelihood that the referral management approach does not present value for money.
Conclusions and Recommendations/cont. • GP commissioning consortia are the obvious conduit for peer review and audit. • There is little evidence to support the ‘passive’ use of clinical guidelines. • The use of financial incentives can be effective, but a blanket reductions in referral rates may lead to a reduction in necessary (as well as unnecessary) referrals.
Messages for GP Commissioners: • Changing referral behaviour is a major change-management task - requires strong clinical leadership from both primary and secondary care • Any strategy to reduce over-referral is likely also to expose under-referral • Reductions in referrals from one source can be negated by rises in referrals from other sources Therefore… • A whole-systems strategy will be required to manage demand, with active collaboration between primary, secondary and community care services
Summary The most cost and clinically effective strategy appears to be built around: • Peer review • Audit • Consultant feedback • Clear referral criteria • Evidence-based guidelines