Download

1 / 32
450 likes | 1.27k Views
Pituitary tumors. By Dr. Abdelaty Shawky Dr. Gehan Mohamed. Optic chiasma. hypothalamus. pituitary.

E N D
Pituitary tumors By Dr. Abdelaty Shawky Dr. Gehan Mohamed
Optic chiasma hypothalamus pituitary
Close examination of a sectioned pituitary gland reveals two closely apposed, but distinctive tissues called the adenohypophysis (anterior or glandular pituitary) and neurohypophysis (posterior or neural pituitary).
Microscopic examination of the conventionally-stained adenohypophysis reveals three distinctive cell types called acidophils, basophils and chromophobes. • This pattern of staining reflects the chemical character of intracellular hormone-laden granules within the pituitary cells.
The neurohypophysis is an extension of the hypothalamus. It composed of bundles of axons from hypothalamic neurosecretory neurons intermixed with glial cells.
Acidophilshave cytoplasm that stains red or orange • Basophils have cytoplasm that stains a bluish color • Chromophobeshave cytoplasm that stains very poorly
1. Acidophils Cells: • Somatotropeswhich produce growth hormone • Lactotropeswhich produce prolactin. 2. Basophils Cells: • Thyrotropeswhich produce thyroid stimulating hormone • Gonadotropeswhich produce luteinizing hormone and follicle-stimulating hormone • Corticotropeswhich produce adrenocorticotrophic hormone
3. Chromophobe cells: - These are cells that have minimal or no hormonal content. Many of the chromophobes may be acidophils or basophils that have degranulated and thereby are depleted of hormone. Some chromophobes may also represent stem cells that have not yet differentiated into hormone-producing cells. • Although classification of cells as acidophils or basophils is useful in some situations, specific identification of anterior pituitary cells requires immunostaining for the hormone in question.
Pituitary adenomas are responsible for about 10% of intracranial neoplasms. • Discovered incidentally in up to 25% of routine autopsies. • In fact, using high-resolution computed tomography or magnetic resonance imaging suggest that approximately 20% of "normal" adult pituitary glands harbor an incidental lesion measuring 3 mm or more in diameter, usually a silent adenoma.
Pituitary adenomas are usually found in adults, with a peak incidence from the thirties to the fifties. • Most pituitary adenomas occur as isolated lesions. In about 3% of cases, however, adenomas are associated with multiple endocrine neoplasia (MEN) type 1 . • Pituitary adenomas are designated, somewhat arbitrarily, microadenomas if they are less than 1 cm in diameter and macroadenomas if they exceed 1 cm in diameter.
* Gross features: • The common pituitary adenoma is a soft, well-circumscribed lesion that may be confined to the sellaturcica. Larger lesions typically extend superiorly into the suprasellar region, where they often compress the optic chiasm and adjacent structures, such as some of the cranial nerves . • As these adenomas expand, they frequently erode the sellaturcica and may also extend locally into the cavernous and sphenoid sinuses.
In up to 30% of cases, the adenomas are not grossly encapsulated and infiltrate adjacent bone, dura, and (rarely) brain, but they do not demonstrate the ability for distant metastasis. • Such lesions are termed invasive adenomas. Foci of hemorrhage and necrosis are common in larger adenomas.
Pituitary adenoma: -This massive, nonfunctional adenoma has grown far beyond the confines of the sellaturcica and has distorted the overlying brain. - Nonfunctional adenomas tend to be larger at the time of diagnosis than those that secrete a hormone.
* Microscopic examination: • Histologically, pituitary adenomas are composed of relatively uniform, polygonal cells arrayed in sheets or cords. Supporting connective tissue, or reticulin, is sparse, accounting for the soft, gelatinous consistency of many of these lesions. • The nuclei of the neoplastic cells may be uniform or pleomorphic. • The cytoplasm of the constituent cells may be acidophilic, basophilic, or chromophobic, depending on the type the cells, but it is generally uniform throughout the cytoplasm. • The functional status of the adenoma cannot be reliably predicted from its histologic appearance.
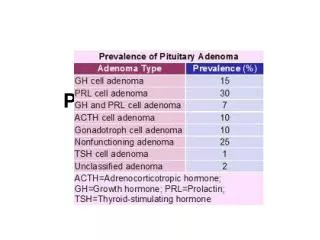
* Classification of Pituitary Adenomas: • Prolactin cell (lactotroph) adenoma. • Growth hormone cell (somatotroph) adenoma. • Thyroid-stimulating hormone cell (thyrotroph) adenoma. • ACTH cell (corticotroph) adenoma. • Gonadotroph cell adenoma.
* Clinical picture: • The signs and symptoms of pituitary adenomas include: a. Endocrine abnormalities: The abnormalities associated with the secretion of excessive quantities of anterior pituitary hormones are mentioned below, when we describe the specific types of pituitary adenoma. b. Local mass effects: May be encountered in any type of pituitary tumor. These include visual field abnormalities, signs and symptoms of elevated intracranial pressure, and occasionally hypopituitarism.
PROLACTINOMA • Prolactinoma(lactotrophadenoma) are the most frequent type of pituitary adenoma, accounting for about 30%. • These lesions range from small microadenomas to large, expansiletumors. • prolactinemia, causes amenorrhea, galactorrhea, loss of libido, and infertility.
Hyperprolactinemia may result from causes other than prolactin-secreting pituitary adenomas. • Physiologic hyperprolactinemiaoccurs in • Pregnancy. • Lactation. • Stress. • Pathologic hyperprolactinemia can also result from lactotrophhyperplasia.
Prolactinomas are treated by surgery or, more commonly, with bromocriptine, a dopamine receptor agonist, which causes the lesions to diminish in size.
GROWTH HORMONE (SOMATOTROPH CELL) ADENOMA • GH-secreting tumors are the second most common type of functioning pituitary adenoma. • Clinical manifestations: • Persistent hypersecretion of GH stimulates the hepatic secretion of insulin-like growth factor I (IGF-I or somatomedin C), which causes many of the clinical manifestations.
If a somatotrophic adenoma appears in children before the epiphyses have closed, result in gigantism. This is characterized by a generalized increase in body size with disproportionately long arms and legs.
If the increased levels of GH are present after closure of the epiphyses, patients develop acromegaly. In this condition, growth is most conspicuous in skin and soft tissues; viscera (thyroid, heart, liver, and adrenals); and bones of the face, hands, and feet. Enlargement of the jaw results in protrusion (prognathism) with broadening of the lower face. The hands and feet are enlarged with broad, sausage-like fingers. • These changes develop for decades before being recognized, hence the opportunity for the adenomas to reach substantial size.
GH excess is also correlated with a variety of other disturbances, including diabetes mellitus, generalized muscle weakness, hypertension, arthritis, congestive heart failure, and an increased risk of gastrointestinal cancers.
Pituitary carcinomas • Pituitary carcinomas are rare, making up some 0.2% of all pituitary tumors, but represent a particular challenge to clinical practice. • The diagnosis of a pituitary carcinoma requires evidence of metastatic disease, either outside the central nervous system (CNS) or as separate noncontiguous foci within the CNS.