Download
1 / 50
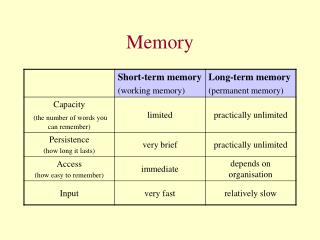
500 likes | 797 Views
Memory. Chris Rorden Anterograde Amnesia Short vs Long Term Memory Episodic vs Procedural Memory Confabulation. www.mricro.com. HM. Severe epilepsy, treated with surgery to bilaterally remove medial temporal lobes. Operation 9/1953, 27 years old Tested 4/1955, age 29

E N D
Memory • Chris Rorden • Anterograde Amnesia • Short vs Long Term Memory • Episodic vs Procedural Memory • Confabulation • www.mricro.com
HM • Severe epilepsy, treated with surgery to bilaterally remove medial temporal lobes. • Operation 9/1953, 27 years old • Tested 4/1955, age 29 • Reported date as 3/1953, age of 27 • No memories since operation • IQ better than pre-op (112) • Fewer seizures • Profound failure to create new memories • Can’t find new home (after 10 mos.) • Can’t remember new people, names, tasks
HM • Deficits • Complete loss of episodic memory • Events/People since operation • Location of new home • Rey figure: copy but not recalled • Semantic memory • Language essentially frozen in 50’s (Gabrieli et al. 1988) • Exceptions: ayatollah, rock ‘n roll
HM – severe anterograde amnesia • Anterograde amnesia – since lesion • Suggests encoding deficit • Retrograde amnesia – prior to lesion retrograde anterograde Memory 1/9/1953 1945 1950 1955
HM working memory • Intact working memory • Normal digit span (remembering numbers) • Wickelgren (1968) showed rate of forgetting within normal range • Unless interrupted (constant rehearsal)
HM procedural memory • Intact procedural memory • Can learn new motor tasks • Mirror tracing task (Milner 1962, 1965) • Pursuit rotor tracing (Corkin, 1968) • Implicitly familiar w testing equipment • Anterograde amnesics can learn new piano pieces (Starr & Phillips, 1970)
HM implicit memory • Perhaps procedural tasks tap ‘implicit’ memory – HM has deficit of ‘explicit’ memory • Milner et al (1968) showed HM learned Gollin incomplete picture task
HM implicit memory • HM has also implicitly learned Tower of Hanoi game (Cohen, 1984). • Can not remember playing, but solves quickly. • Start Position • Goal 2 (2 moves) • Goal 10 (5 moves)
Memento – Amnesia in Film Noir • Guy Pierce • Sammy Jenkins
HM • Temporally graded retrograde amnesia • Old memories (childhood) OK • Memories immediately before lesion lost • Forgot death of favourite uncle in 1950 • Suggests consolidation takes time Memory 1/9/1953 1945 1950 1955
How long does consolidation require? • Testing retrograde amnesia. • HM: photos of celebrities suggest retrograde amnesia spans decades, with more distant memories relatively preserved (Marslen-Wilson & Teuber, 1975) • PZ – Butters & Cermak (1986) • Wrote autobiography • Test personal memories
Medial Temporal Lobe Memory • MTL patients • Short term memory intact • Old long term memory intact • Suggests ‘consolidation’ deficit • ‘Encoding’ deficit, retrieval intact • See Warrington & Weiskrantz for alternate view • Unable to create new LTM • LTM formation requires years?
Anatomy • Anterograde amnesia follows damage to medial temporal lobe or connected regions. • MTL or diencephalic structures like thalamus and mamillary bodies • E.G. NA had fencing foil in nose • Accident in 1960 • Diencephalic damage • Similar to HM, though less retrograde
Anterograde Amnesia Similar deficits with damage anywhere in Papez circuit. Fornix (Squire’s Patient) Mammillary body (Korsakoff Patients) Hippocampal formation - HM
Hippocampus (T1 MRI) • Folded shape seen in coronal image. • Here: healthy individual
HM’s lesion • Surgeon report describes removal of entire hippocampus (Scoville & Milner, 1957). • Recent MRI (Corkin et al., 1997) study suggests posterior hippocampus is present (though atrophied). Scoville & Milner 1957 Corkin et al. 1997
HM’s lesion • Corkin et al. (1997) • bilaterally symmetrical • medial temporal pole • most of the amygdaloid complex • most or all of the entorhinal cortex • anterior half of hippocampal formation (dentate gyrus, hippocampus, and subicular complex)
Memory – primacy and recency • People often remember the first few and last few items in long lists • First words: primacy – most rehearsal • Final words: recency – least interference • Clearly easier: you do not have to remember as long • These are thought to reflect different processes % recall 1 2 3 4 5 6 7 8 9 10 Item Number
Amnesics show no primacy effect • Patients like HM remember last few words (when not interrupted) • Recency effect intact • Primacy effect gone: no encoding benefit % recall 1 2 3 4 5 6 7 8 9 10 Item Number
Memory • Are primacy and recency effects different processes • Maybe recency is simply easier • Evidence would come from patients who show an opposite pattern of effects: • Primacy intact • Recency impaired • These patients would provide a ‘double dissociation’
Primacy and recency Short term (working) memory Long term memory % recall 1 2 3 4 5 6 7 8 9 10 Item Number
Patient KF • Shallice & Warrington (1970) • Primacy effect intact • Recency effect impaired • Complements amnesic patients % recall 1 2 3 4 5 6 7 8 9 10 Item Number
Potential Paradox Can information get into long term memory if there is no short term memory? Short term memory Long term memory % recall 1 2 3 4 5 6 7 8 9 10 Item Number
Does LTM require STM? • According to Atkinson & Shiffrin (1968) • STM rehearsal leads to LTM • Predicts that LTM will depends on STM • Can not accommodate Shallice and Warrington’s patient Sensory (iconic) Memory Short Term Memory Long Term Memory
Shallice & Warrington (1970) • S & W suggest that short term and long term memory independent from each other. • Short term memory not required for long term memory • Very controversial model
Baddeley working memory • STM is encoded by system dedicated to input • Verbal info: phonological loop • Visual info: visuo-spatial scratchpad • LTM is more modality independent Phonological Loop Visuo-Spatial Scratch pad Phonological Loop Long Term Memory
A: Implicit vs explicit memory • MTL amnesics • Explicit memory: unable to create • Implicit memory: relatively intact • So far: single dissociation • 2 possibilities: • Implicit/Explicit 2 independent systems • Implicit simply easier, relies on residual processing of a single, partially damaged system • Double dissociation would support claim of 2 independent systems
B: Gabrieli et al. (1995) • Patient MS • 29 year old, right handed male • Intractable epilepsy: surgery removed right BA 17,18, part of 19. • Hemianopic (blind in left field) • Compared to MTL amnesics and healthy controls.
C: Results • Explicit memory task • Shown 24 words, later shown 48 words (24 from 1st phase, 24 new foils): asked to say if words were previously seen. • Amnesics poor. • MS fine.
D: Conclusion • Implicit memory: word completion task • Shown/Heard 24 words ‘stick’, later asked to complete 48 stems, 24 could be solved with items from 1st phase (‘sti__’) and 24 unrelated stems (‘sta__’). • Healthy people show priming effect (faster if solution seen previously). This effect is much bigger if words were seen (physical match) rather than heard. • Amensics show normal priming. Shows implicit memory. • MS visual priming is no greater than auditory priming. Therefore, shows no extra benefit for physical match of stem and previously seen word. • Conclusion • Double dissociation • Explicit memory has some distinct processing from implicit memory. • ‘Conceptual’ priming intact in MS, perceptual priming damaged
Recollection vs Familiarity Memory • Is implicit memory really preserved in MTL amnesics? • Explicit tasks usually much harder: • ‘Explicit’ Recall: “What was the picture I showed you earlier?” Could have thousands of answers. • ‘Implicit’ Recognition: “Which of these two pictures did I show you” only has two answers, and seeing the correct answer may jog memory. • Is this a meaningful dissociation? (see Simons & Spiers, 2003) • Jon and YR have intact Recognition, but impaired recall • Selective lesions to only hippocampus or fornix • LG and PH have poor Recognition, even poorer recall • Damage to hippocampus and surrounding parahippocampal regions • Both groups show same pattern • Not a double dissociation • Harder task impaired for everyone
Recollection vs Familiarity Memory • Yonelinas et al. (2002) compare hypoxic patients (H, focal bilateral damage to hippocampus) to patients with unilateral but extensive damage to the hippocampus and surrounding tissue (H+) and controls (C). • For H group, recall correlated with recognition (below, left) • Interaction between groups • H+ poorer at familiarity (poor implicit) • H poorer at recollection (poor explicit) • Suggests Double dissociation is real
Semantic vs. episodic memory • HM has impaired semantic and episodic memory: • Semantic: Language frozen in 1950s (Gabrieli et al.) • Episodic: poor at remembering events. • However, his lesions damage both hippocampus and surrounding temporal lobe. • What about patients with more selective damage?
A: Graham et al. 2000 • Graham et al. suggest double dissociation: • Early Alzheimer's patients • ‘Semantic dementia’ patients Alzheimers Patient Hippocampus atrophy Semantic Dementia Temporal lobe atrophy
B: Test stimuli • A: Semantic naming task (‘phone’) • Correct answer: ‘phone’. Memory tested 30 minutes later: • B: Episodic memory task (perceptually identical) • Correct answer: ‘I saw a phone earlier’ • C: Episodic memory task (perceptually different) • Correct answer: ‘I saw a phone earlier’.
C: Semantic naming • Semantic dementia patients have difficulty naming items. • AD patients are fine at this task.
D: Episodic memory • AD patients • poor episodic memory. • SD patients • OK with identical items • Poor with perceptually different (especially if unable to name item in picture naming phase).
E: Conclusions • Suggests semantic and episodic memory may be separate. • Hippocampal formation: encoding episodic memories • Temporal lobe: storage of semantic memories. • Additional support from Vargha-Khadem (1997), who reports 4 patients with selective hippocampal damage: all show impaired episodic but intact semantic memory. • Note: all sustained hippocampal damage early in life, so does not necessarily generalize to adult brain.
Memory & Prefrontal Cortex (PFC) • PFC damage results in • Disinhibition • Impulsiveness • Disorganization • Memory deficits • Other deficits can hide memory problems • Less ‘pure’ than MTL amnesia • Note: oribtofrontal cortex subdivided: • Ventromedial PFC • Ventrolateral PFC
Memory structure (Squire & Knowlton, 1994) • Simplified from page 349 of Gazzaniga book Declarative memory (explicit) Nondeclarative memory (implicit) Events (episodic) Experiences particular to time/place MTL, PFC Facts (semantic) World/word, language knowledge, conceptual priming MTL, PFC Procedural Motor, cognitive skills Basal ganglia, cerebellum Perceptual Perceptual priming Association cortex
Interaction of different brain regions • Lesions in animals and functional imaging suggest network of regions work together to encode memory. • Beyond scope of neuropsychology course.
Spontaneous confabulation • Confabulation syndrome: • Spontaneously produce confabulations (no need to make things up, no external trigger) • Convinced of accuracy of their confabulations • Acted on confabulations (indication of conviction)
Double dissociation • Spontaneous and provoked confabulation dissociate: Schnider et al. (1996), Brain 119, 1365-1375. • Spontaneous confabulation • Generate false memories without prompting • Often whole gist of memory is false • Provoked confabulation, false recognition: • Can be seen in healthy adults • Accidentally report having seen word earlier in list if it is similar to previous word • Errors with small details of overall story
Example of spontaneous confabulator • 58-year old woman • Aneurysm of anterior communicating artery. • Reported: needed to go home to feed her baby • Her ‘baby’ was 30 years old
Case 2 • 48 year old tax accountant • Traumatic damage to orbitofrontal lobe • Left hospital convinced taxi was waiting to take him to meeting • Consistently thought he had business meeting
Reflections • Ideas tend to be internally consistent but inaccurate. • Careful testing shows they are disoriented, confuse date and time. • When confronted, often search for explanations but fail to adapt their ideas • Patient in Berne convinced he was in Bordeaux. • Admitted view from window inconsistent with belief. • Did not change belief.
Most confabulations about present • Plausible • Traced to actual events • Usually accurate regarding old memories • Majority eventually stop confabulating despite permanent brain injury
Eliciting confabulations • Individual is asked if they saw an image before earlier in run. • Do not report having seen image if you only saw it in a previous run.
Eliciting confabulations • Both amnesics and confabulators do poorly at remembering if they have seen an item before. • Amnesics forget previously seen items. • Confabulators report having seen an image from previous set in current set. • Problem with context, not recognition per se.
Anatomy of t • Patients who spontaneously confabulate tend to have orbitofrontal damage (aka damage to the ventromedial PFC).