Download
1 / 22
300 likes | 829 Views
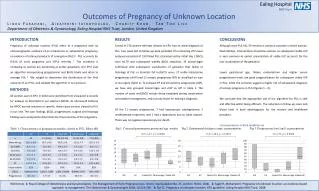
Pregnancy Of Unknown Location (PUL). Dr Kamel Elbadry MD (Sheffield University), FRCOG Consultant Obstetrician and Gynaecologist. ● The term PUL is used whenever there is no sign of either intra or extrauterine pregnancy or retained products of conception on transvaginal ultrasound

E N D
Pregnancy Of Unknown Location (PUL) Dr Kamel Elbadry MD (Sheffield University), FRCOG Consultant Obstetrician and Gynaecologist
●The term PUL is used whenever there is no sign of either intra or extrauterine pregnancy or retained products of conception on transvaginal ultrasound ● A pregnancy site will not be visualised in 8-10% of early pregnancy scan in EPAU, up to 31% in other units
Assessment Whenever a woman presents with a positive pregnancy test but no evidence of pregnancy on TVS, clinical assessment and serum B hCG should be carried out.
hCG and Ultrasound: Using a discriminatory zone of hCG has been widely evaluated. An intrauterine pregnancy should be visible on ultrasound if hCG ranges from 1000-2400 iu/l
In multiple pregnancy, hCG levels should be interpreted with caution as they are little higher, requiring an extra 3 days for the sacs to be visible. • If hCG level above the discriminatory level with no intrauterine gestational sac on ultrasound. Determine whether the pregnancy is ectopic
The diagnosis of ectopic pregnancy should be based on the identification of an extrauterine sac, and indirect signs such as a complex adnexal mass or fluid collection rather than empty uterus on scan. • The combination of the above scan findings has a positive predictive value of 93.5%-100% for diagnosing ectopic.
Trans-vaginal colour Doppler has not been shown to increase the detection rates of ectopic when compared with 2D ultrasound but may be useful in showing enhanced trophoblastic flow.
The discriminatory level of each unit should be based on : hCG assay technique in use Quality of ultrasound equipment Operator experience
Progesterone: Serum progesterone levels are elevated, indicating the viability of corpus luteum, but decrease if the pregnancy fails. Progesterone level < 25 nmol/l, associated with nonviable pregnancy (viable in 0.3%)
Progesterone < 20 nmol/l predicts failing pregnancy with a positive prediction value > 95% Levels > 25 nmol/l are associated with pregnancies. Levels > 60 nmol/l are strongly associated with intrauterine pregnancy (2.6% ectopic)
hCG pattern after 48 hours: ● Rise of hCG by 66%, predicts an intrauterine pregnancy (predictive value 96.5%) ● Fall of hCG by at least 15%, most likely outcome failing pregnancy When the rise or fall in hCG is suboptimal, the most likely diagnosis is ectopic.
Management of PUL Conservative management: According to the Association of Early Pregnancy Units guidelines, if no intrauterine or ectopic pregnancy or retained products of conception are seen on TVS and the woman is asymptomatic she can be managed conservatively.
Expectant management of PUL has been shown to be safe and to reduce the need for unnecessary surgical intervention and is not associated with any serious adverse outcomes. Unfortunately, multiple visits to EPAU are necessary before diagnosis can be made.
Clinical outcome of PUL: 1- Failing PUL (44-69%) 2- Intrauterine pregnancy 3- Ectopic pregnancy 4- Persistent PUL
Persistent PUL: Those in which the serum hCG levels fail to decline and there is no evidence of trophoblastic disease and the location of pregnancy can not be identified. Usually hCG are low (<500 iu/l) and have reached to a plateau (2% of PUL)
Medical Management: Methotrexate, 50 mg/m2 has been used successfully in persistent PUL (90% effective)
Surgical Management: Laparoscopy/ laparotomy is indicated if the woman is symptomatic or if an ectopic is visualised. Laparoscopy has false negative rate 3-4% (if done too early) and false positive 5% because of retrograde uterine bleeding.
Curettage Not a usual practice in UK, although common in USA No clinical evidence to change our practice.
Conclusion Asymptomatic PUL should be managed conservatively as none of the methods to predict the clinical outcome of PUL is 100% accurate. Follow up with hCG and ultrasound until the pregnancy is located or intervention become necessary
Medical management should be reserved for women with asymptomatic persisting PUL Surgery is indicated if the woman is symptomatic