Download
1 / 27
270 likes | 409 Views
New treatments for CF. Peter D. Sly MBBS, MD, FRACP, DSc. Early intervention in CF. What are we trying to achieve? Who should be treated? What are the treatment options? What is the evidence that early intervention works?. Early intervention in CF. What are we trying to achieve?

E N D
New treatments for CF Peter D. Sly MBBS, MD, FRACP, DSc
Early intervention in CF • What are we trying to achieve? • Who should be treated? • What are the treatment options? • What is the evidence that early intervention works?
Early intervention in CF • What are we trying to achieve? • CF lung disease begins early and is progressive Sly et al NEJM 2013
Persistence of Bronchiectasis 301 paired scans 1y apart from 143 children (0.2-6.5y). Bx persistent in 73% and extent increased in 63% Progression in 63% Mott Thorax 2012
Gas trapping on CT • What does Gas trapping mean? • Uneven emptying of lung units • Is it associated with disease? • Increases risk of bronchiectasis [Sly NEJM 2013] • Weak association with M2/MO but not LCI [Hall PLoS ONE 2011;6:e23932] • Can it be treated? • No data in infants
Who should be treated? Absence of symptoms does not mean absence of disease
What are the treatment options? • Treatment options depend on disease mechanisms • Inflammation: anti-inflammatories • Infection: antibiotic prophylaxis • Thicker mucus: mucolytics • Dehydrated ELF: HS, eNaC blockers • Impaired mucociliary clearance: HS, DNAse • Impaired anti-oxidant defence: anti-oxidants; GSH • Gene defect: gene therapy, CFTR correctors, potentiators
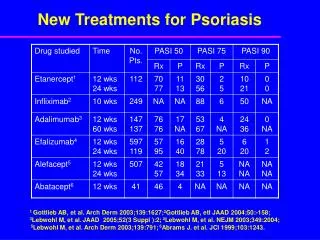
Non-steroidal anti-inflammatories • Cochrane Review (Lands & Stanojevic 2013, Issue 6) • 5 trials (3 IBP), 334 subjects 5-39y, max 4y FU • Data in children: • Konstan 1991: 13 IBP, 5 placebo; 300/400/600mg BD • Konstan 1995: 42 IBP, 43 placebo; 20-30mg/kg • Lands 2007: 142 (6-18y); 20-30 mg/kg • Outcomes • Reduced decline in lung function (combined analyses) • FEV1% mean dif 1.16 [0.07-2.25] – NS >13y • FVC% 1.27 [0.26-2.28] – NS >13y • FEF25-75% 1.72 [0.10-3.34] – NS >13y
Prophylactic anti-staph antibiotics • Cochrane review [Smyth & Walters 2012, Issue 12] • 4 studies, 401 children 0-7y randomized • Fewer children with ≥1 isolation of Staph • But: • Complete eradication not achieved in most • No difference in: • Isolation of other microbes • Lung function (infant or spirometry) • Nutrition (weight or height) • Hospitalization, days in hospital, other antibiotics • CXR score
Dornasealfa • Major results form studies in adults: • Improved lung function/ decreased rate of decline • Decreased exacerbations • Improved QOL • Pulmozyme Early Intervention Trial (PEIT)
FEV1 % predicted Quan J Pediatr 2001; Robinson PediatrPulmonol 2002
Dornasealfa • Impact on ventilation inhomogeneity and gas trapping • 17 children (6-18y, mean 10.32y), FEV1≥80% • 4w cross-over, placebo-controlled • Dornasealfa: • Improved LCI 0.90±1.44; p=0.022, FEF25-75 6.1%±10.34% [Amin, ERJ 2011;37:806-812] • 25 children (6-18y), FVC ≥85%, FEV1≥70% • 12m placebo-controlled RCT • Improved gas trapping: • 3m 13% v 48%, p=0.023; 12m 15% v 61%, p=0.053 [Robinson Chest 2005;128:2327-35]
Hypertonic saline • Major results from adult studies • Improved lung function / decreased rate of decline • Reduced acute exacerbations / improved QOL • Increased mucociliary clearance • Inhaled HS in infants and children <6y (ISIS)
Hypertonic saline No reduction in exacerbations; 40% of subjects on dornasealfa Rosenfeld JAMA 2012;307:2269-77
Hypertonic saline • Impact on ventilation inhomogeneity • 20 children (6-18y, mean 10.5); FEV1 96±12% • Cross-over; 4 week treatment (HS/P), 4w wash-out • Decreased LCI; 1.16±0.94 (0.27-2.05), p=0.016 • No change in spirometry, QOL [Amin Thorax 2010;65:379-83]
Hypertonic saline • Impact on mucociliary clearance • 12 children (8.9-12.4y), FEV1108%, single dose 7% HS • MC by radio-aerosol clearance • Improved MC in some, esp if low at baseline Laube BMC Pulm Med 2011;11:45
Dornasealfa v hypertonic saline • 14 children, mean age 13.3y, FEV1 75.6% • 3 w treatment (D 2.56mg/HS 5.85%), 3w WO • FEV1 HS 7.7% (14%) v D 9.3% (11.7%), p<0.05 Ballmann JCF 2002
Azitromycin AZM: ↑ lung function, QOL, wt gain , ↓ exacerbations
Azitromycin • Potential mechanisms • ↓ neutrophilic inflammation • ↑ anti-oxidant defences • ↓ viral LRI • Prevent “pro-inflammatory” microbiome
Azitromycin • ↓ neutrophilic inflammation • Most evidence from erythromycin in DPB • ↓ pro-inflammatory cytokines • BEC, neutrophils, monocytes • ↓neutrophil accumulation • Inhibit ICAM-1, ↓ IL-8, ↓ migration • ? ↓ neutrophil activation • ↓ NE [KanohClin Micro Rev 2010; Frielander Chest 2010]
Azitromycin • ↑ anti-oxidant defence • ↓ neutrophilic inflammation → MPO → ↓ OS • AZM prevents OS-induced upregulation of GSTs • Catalyses oxidation of GSH to detoxify oxidants • Further ↓ available GSH [Bergamini AJRCMB 2009]
Azitromycin • ↓ viral LRI • AZM → ↓ exacerbations in RCTs • AZM → ↑ HRV-induced IFN, ↓ HRV replication in AEC • ? ↓ spread of virus from URT to LRT [Gielen ERJ 2010; Zaheer AJRCMB 2010]
Gene potentiators/correctors Kreindler. Pharmacology & Therapeutics Volume 125, Issue 2 2010 219 - 229
Ivacaftor • Potentiates opening of CFTR channel with G551D • “normalizes” sweat chloride • improves lung function • Improves nutrition • Case study: 7y girl G551D/G551D
5m pre ivacaftor 7 months of ivacaftor pre ivacaftor 11 months of ivacaftor
New options in clinical trial • Lumacaftor • Gene corrector – “escorts” CFTR to cell surface (F508) • Ataluren • Allows read through premature stop codon • Neutrophil elastase inhibitors • ONO-6818; AZD9668
Early intervention in CF • Summary • Lung disease begins early in CF • Lack of symptoms does not mean no disease • Treatment must start early to prevent disease • Lack of RCTs in infants to guide treatment