Download
1 / 27
410 likes | 1.22k Views
Defibrillator, pacemakers and icd. Presented by: rashmi bhatt Moderator: dr dara negi. objectives. Principle of defibrillator Defibrillator vs cardioversion Principle and working of pacemaker Anesthetic implications Functioning of ICD Anesthetic implications of ICD. Defibrillation.

E N D
Defibrillator, pacemakers and icd Presented by: rashmibhatt Moderator: drdaranegi
objectives • Principle of defibrillator • Defibrillator vscardioversion • Principle and working of pacemaker • Anesthetic implications • Functioning of ICD • Anesthetic implications of ICD
Defibrillation • Non synchronised delivery of energy during any phase of the cardiac cycle • Indications : VT, VF, cardiac arrest due to or resulting in these • Avoided in dysarrythmias d/t digitalis toxicity or catecholamine induced overactivity • Generally under induction or sedation unless patient is hemodynamically unstable • Hand held paddles considered better than self adhesive electrodes
DEFIBRILLATOR • Types : AED, semi automated,standard with monitor and implantable • Positioning: anterolateral and anteroposterior • Anterolateral: left 4/5 ICS in midaxillary line and right sternal edge in 2/3 ICS • Anteroposterior: right sternal edge 2/3 ICS and b/w tip of left scapula and spine • Anteropost is more effective for AF and preferred in pts with implantable devices
Energy selection • Energy wave forms: monophasic and biphasic • Biphasic: truncated and rectilinear • Biphasic is more effective and uses lesser energy • Atrial flutter: 25-50 J; AF: 50-100 J in stable patients • Polymorphic VT(unstable) or VF: 200-360 J • Monomorphic VT(stable): 100-200 J • In pediatric patients: 0.5J/kg • Complications: arrythmias(VF), thromboembolism(esp in AF), myocardial necrosis, ST elevation ( for upto 2 min), painful skin burns,hypoxia and rarely pulmoedema. Also injuries to the health care personnel.
cardioversion • Delivery of energy is synchronised to the large R waves or the QRS complexes • Indications: SVT, AF, atrial flutter, vent tachy, reentrant tachy with hemodynamic instability • Synchronization is in the early part of QRS • Internal cardioversion: preceded by anticoagulation. Three temp catheters are inserted under fluoroscopic guidance. Two are used to deliver the shock and the third for R wave synchronisation and pacing. • 1st in distal coronary sinus, 2nd in rt atrium appendix or lateral wall, both being connected to external defibrillator. 3rd(quadripolar) in apex of rt ventricle, connected to external pacemaker. Energy delivered is 5.6+-4.7 J.
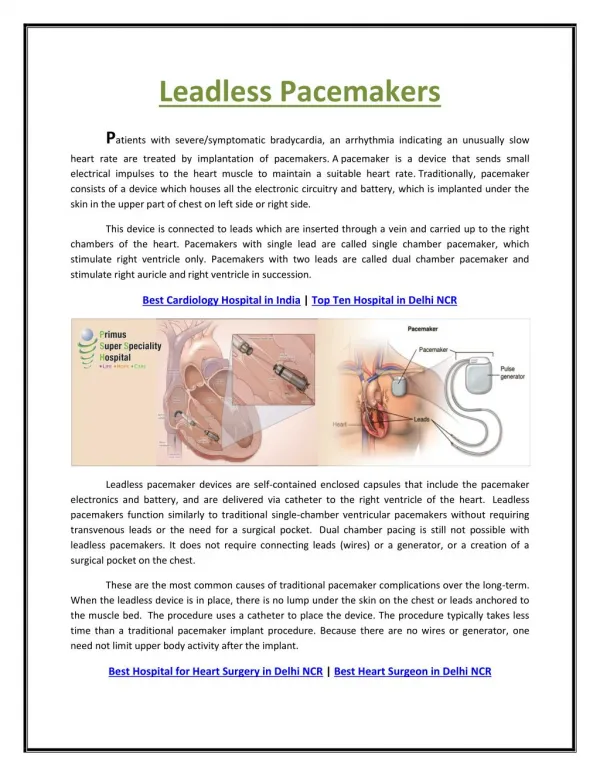
pacemaker • Temporary or permanent • Consists of an impulse generator and lead(s) • Leads could be transvenous or epicardial in position, uni, bi or mutipolar in no of electrodes • Unipolar: more sensitive to EMI, gas interference • Bipolar uses less energy and more resistant to interference • Placement could be transthoracic, transvenous or transesophageal
Indications: sinus node disease, av node disease, long QT syndrome, HOCM, DCM • Magnet behaviour: not all devices are sensitive • Magnet response: IFI/ERI/EOL • Some pacemakers carry out TMT • Pacemaker induced tachycardia
Anaesthetic implications • Pre op: optimise coexisting diseases, CXR, reprogramming (to prevent oversensing). Spl considerations in lithotripsy, hysteroscopy, chest/abd procedures, TURP,ECT etc. • intraop: ecg filtering disabled, avoid monopolar ESU, equipment for pacing, defibrillation to be ready. • Post op: reprogramming and reinterrogation. • Pacemaker failure: generator failure, lead failure, failure of capture • Failure of capture may result from increase in the threshold for capture • Correction by magnet application, temporary pacing, sympathomimetic drugs(epi/dopa).
Implantable cardioverter- defibrillator • Important to differentiate from other thoracic devices esp pacemaker in v/o electromagnetic interference(EMI) • Previously placed in an abdominal pocket; present day pectoral placement • Can be differentiated using a CXR to examine the RV lead system. • Other devices could be for pain control, thalamic stimulation to control PD, phrenic nerve stimulation, vagus stimulation for epilepsy, depression, heart failure and obesity.
Battery powered device to deliver energy in form of shock to terminate VT/VF • Believed to be superior to drug therapy in pt with EF<35% • Average life of 3-6 years • Principle: measures R-R interval and categorises as normal, fast or slow. • Programmed to confirm VT/VF to avoid inappropriate therapy(mc SVT) • Delivers 6-18 shocks per minute • Programmed to diff VT from SVT by onset, stability, QRS width, AV synchrony and waveform • In case of slow R-R, antibradycardia pacing
Techniques of icd placement Tranvenous or endocardial approach Surgical or Epicardial approach
Indications: vent tachy, vent fib, pts awaiting heart transplant, long QT syndrome, brugada syndrome, RV dysplasia. • Prophylactic role in HOCM, post MI with EF<30% • Magnet behaviour: suspension pfantitachycardia pacing. Generally no effect on antibradycardia pacing.
Anaesthetic implications • Pre op: optimisation of coexisting conditions checking of battery life disable antitachycardia therapy CXR to confirm position of RV lead • Intra op: ecg monitoring facility to deliver external cardioversion/defibrillation • Post op: reinterrogation and reenabling