Download
1 / 82
840 likes | 1.36k Views
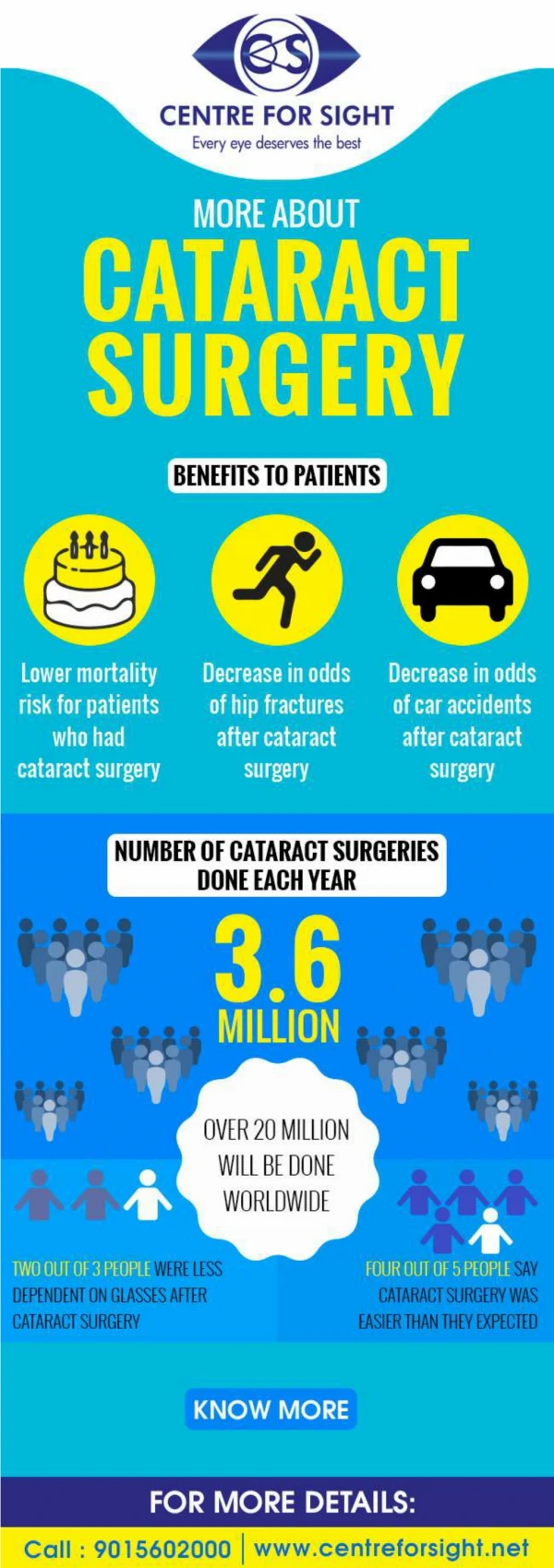
Cataract Surgery in the Developing World. Dr Brad Townend BSc(Med), MBBS, MPH, MMED, FRANZCO. A Blinding Problem…. Cataract is the leading cause of blindness in the world Defined as VA <6/120 More than 20 million people in the world ‘blind’ due to cataract

E N D
Cataract Surgeryin theDeveloping World Dr Brad Townend BSc(Med), MBBS, MPH, MMED, FRANZCO
A Blinding Problem… • Cataract is the leading cause of blindness in the world • Defined as VA <6/120 • More than 20 million people in the world ‘blind’ due to cataract • 1999: International Agency for the Prevention of Blindness (IAPB) and the World Health Organization (WHO) “Vision 2020: The Right to Sight” initiative. • Mission: sustainable provision of high-quality cataract surgical services throughout the underdeveloped world. • At the start: number of people blinded by cataract projected to double by year 2020 if no improvements in global eye care delivery • Significant progress has been made in quantity and quality of cataract surgery provided in Developing World
Q1: What is the leading cause of blindness in the world? A Cataract B Glaucoma C AMD D Infection / Uveitis
Intracapsular Surgery • No IOL technology • Large wound • Zonule dissolving solution, cryo probe • Time consuming surgery • Ocular complications significant • RD, CMO, expulsive haemorrhage, infection • Significant morbidity (weeks in hospital) • Remain aphakic with spectacle correction
Harold Ridley • WWII Royal Air Force casualties • Splinters of plastic (acrylic) from shattered aircraft cockpit canopies became lodged in the eyes of wounded pilots • Inert (did not trigger rejection or inflammation) • artificial lenses for cataract surgery • Much opposition from the medical community initially • Finally approved by FDA as ‘safe and effective’ for human use in 1981
Q2: Harold Ridley implanted the first IOL in 1950 made of what material? A Glass B Silicon C Quartz D Acrylic / Perspex
Extracapsular Surgery • Preserve capsule for IOL insertion • 10 mm limbal incision (astigmatism) • 8-10 sutures • Astigmatism, time, suture removal, complications • Slow visual rehabilitation
Phaco-Emulsification • Better refractive and visual outcomes • Quicker surgical time (sutureless) • Fewer complications • Fast rehabilitation BUT • High cost of equipment • Maintenance • Consumables • Most blind people live in developing world
Q3: Which of the following is a disadvantage of phaco-emulsification over traditional extracapsular surgery? A Faster rehabilitation time B Astigmatism C Cost D No need for sutures
SICSSmall Incision Cataract Surgery • Good quality outcomes • Cheap ($20 AUD per case) • Cheap tools • Cheap lenses • No phaco machine • Few consumables (except blades) • Efficient surgical times (5 minutes) and turnaround times (3 minutes) • Sutureless • Much easier and quicker to learn than phaco • More forgiving than phaco when complications • Particularly for difficult dense cataracts • Can’t do SICS on soft Western cataracts! • Much fewer post-op visits than ECCE • Better VA outcomes than ECCE, and almost as good phaco
Q4: Which of the following is a limitation of SICS surgery? A Cheap B Difficult to perform on soft Western cataracts C Efficient surgical times D Astigmatism
OUTCOMES: SICS vsPhaco in Developing World • 3 RCT’s • Phaco: more corneal oedema on day 1 post-op with worse VA on day 1 • No significant difference in endothelial cell loss between techniques at 6 weeks • Phaco had higher rates of UCVA >6/9 and BCVA >6/6 compared to SICS • At 6 months: rate of BCVA and UCVA >6/18 similar between phaco and SICS • Phacotook 15.5 mins on average, SICS took 9 mins • PCO rate significantly higher in SICS group at 6 months (but VA not worse!) • Needs longer follow-up • Complication rates (including endophthalmitis) similar • BUT: • SICS more efficient and economical • SICS faster visual rehabilitation (For treating advanced cataracts in the Developing World)
Q5: Which of the following is true for treating advanced cataracts in the Developing World? A SICS is more efficient, economical and has outcomes that are just as good as phaco B SICS causes more corneal oedema than phaco C Phaco has quicker post-op rehabilitation D SICS has more complications
References • Gogate P, Deshpande M, Nirmalan PK. Why do phacoemulsification? Manual small-incision cataract surgery is almost as effective, but less expensive. Ophthalmology. 2007;114:965–968. • Gogate PM, Kulkarni SR, Krishnaiah S, et al. Safety and efficacy of phacoemulsification compared with manual small-incision cataract surgery by randomized controlled clinical trial. Ophthalmology. 2005;112:869–874. • Ruit S, Tabin G, Chang D, et al. A prospective randomized clinical trial of phacoemulsification vs manual sutureless small-incision extracapsular cataract surgery in Nepal. Am J Ophthalmol. 2007;143:32–38. • Ruit S, Tabin GC, Nissman SA, Paudyal G, Gurung R. Low-cost high-volume extracapsular cataract extraction with posterior chamber intraocular lens implantation in Nepal. Ophthalmology. 1999;106:1887–1892. • Tabin G, Chen M, Espandar L. Cataract surgery for the developing world. CurrOpinOphthalmol. 2008;19:55–59.