Download
1 / 59
590 likes | 777 Views
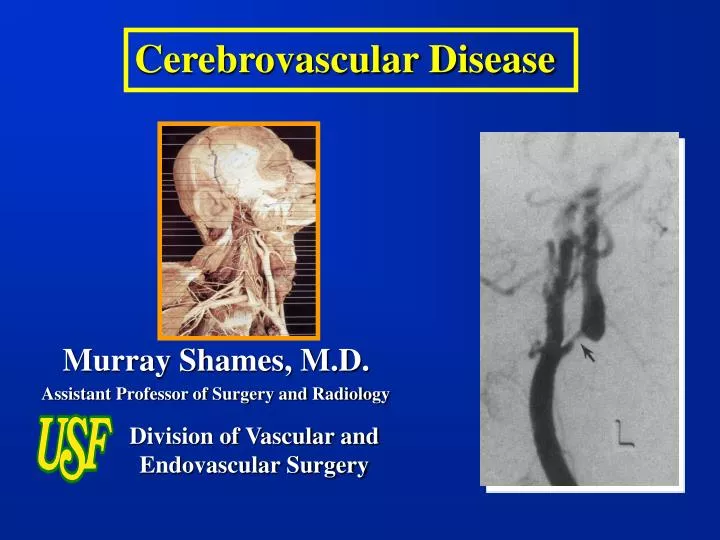
Division of Vascular and Endovascular Surgery. Murray Shames, M.D. Assistant Professor of Surgery and Radiology. Fundamentals :. Stroke is the third leading cause of death in the USA (200 000) Incidence 160/100 000 HTN most common cause 30% associated with extracranial carotid stenosis

E N D
Division of Vascular and Endovascular Surgery Murray Shames, M.D. Assistant Professor of Surgery and Radiology
Fundamentals: • Stroke is the third leading cause of death in the USA (200 000) • Incidence 160/100 000 • HTN most common cause • 30% associated with extracranial carotid stenosis • Significant disability $7.5 billion (1976)
Relative Risk for Ischemia: • Age: • 10/100,000 < 45 yr • 1000/100,000 > 75 yr • Hypertension: 6x • Atrial fibrillation: 6x • Prior stroke/TIA: 5 x • Asymptomatic carotid bruit: 3x • Smoking: 2x
Pathology: Carotid Artery Lesion 90 % atherosclerosis 10% fibromuscular dysplasia, intimal dissection, inflammatory lesions, radiation
Atherosclerosis: • Similar L-R distribution • 40% of lesions at proximal ICA • 20% of lesions at proximal vertebral • Aortic arch disease in 10% of patients
Other causes of stroke: • Cardiac embolus • atrial fibrillation • heart valve disease • Rupture of intracranial aneurysm • Intra-cranial hemorrhage • Carotid artery dissection • Carotid aneurysm • Fibromuscular dysplasia • Radiation
Fibromuscular Dysplasia: • Carotid second most common site of disease • 92% Women • 30% of patients intracranial aneurysms • Degenerative process involving long, unbranched medium sized vessels • Hormonal, mechanical, unusual distribution of vasa vasorum • Histology • Intimal fibroplasia • Medial Hyperplasia • Medial Fibroplasia (most common)- replacement of media with dense fibrous connective tissue • Perimedial dysplasia (renals)
Carotid Dissection: • Traumatic disruption of intima • Compression of true lumen
Pathogenesis of Atherosclerosis: • Intimal injury (hemodynamics) • Nodular deposition of fat in arterial intima • Associated inflammatory response – fibroblast, smooth muscle cell proliferation • Slow accumulation of lipoproteins • Calcium precipitation in the primary fatty plaque.
Hemodynamics: • High shear stress • Turbulent flow • Flow seperation • Propensity for outer wall opposite flow divider
Atherosclerosis: • Flow reducing • Embolic • Clot • Platelets • Cholesterol debris • Thrombosis
Complex Carotid Plaques: • Calcification • Loss of intimal continuity • Ulcer formation • Subintimal necrosis • Plaque hemorrhage
Presentation: • Asymptomatic • Transient Ischemic Attacks • Cerebral Infarction
Asymptomatic: • Natural history- progression of disease • >80% stenosis associated with 35% risk of symptoms or occlusion in 6 months
Surveillance: Duplex scan q 6-12 months
Transient Ischemic Attacks: • reversible, painless neurologic deficit, lasting 1-5 minutes • Complete recovery < 24 h
Transient Ischemic Attacks: • a harbinger of stroke (30-40% of patients with surgically accessible carotid stenosis) • No loss of consciousness - syncope • Amaurosis fugax: embolus to ipsilateral retinal artery • Aphasia • Contralateral paralysis, paresis, paresthesias • Stroke rate at 1 ,3 , 5 years 23%, 27%, 45% • Crescendo TIA’s/ Stroke in evolution
Stroke: • Brain infarction • 50% preceded by TIA • Embolic or thrombosis with inadequate collaterals • Symptoms greater than 24 hours • 1/3 resolve, 1/3 deteriorate, 1/3 remain the same
Sequalae of Internal Carotid Artery Occlusion: • propagation of thrombus to intracranial arteries • embolization of thrombus • both can result in cerebral infarction • outcome depends on adequacy of collateral flow: Circle of Willis
‘VIRULENCE’ OF CAROTID ARTERY DISEASE BASED ON CLINICAL SYMPTOMS Clinical entity Risk of subsequent stroke Recent (< 4 mo) stroke High (10-15%) Recent hemispheric TIA unstable plaque Recent amaurosis fugax Previous stroke, TIA, amaurosis Silent infarct CT or MRI Asymptomatic bruit Low (1-3%) Non-hemispheric symptoms Hypertension
Clinical Evaluation: • History and Physical Exam • Degree, duration of symptoms • Extent of recovery • Presence of infarction on CT/MRI • Cerebrovascular Imaging • Duplex • Angiography • MRA
Velocity Criteria: PSV, ICA/CCA Ratio: • >50 % stenosis: PSV > 125 cm/sec ICA/CCA ratio>2.0 • >60% stenosis: PSV > 230-270 cm/sec ICA/CCA ratio>3.5 • >70 % stenosis: PSV > 290-325 cm/sec ICA:CCA ratio>4.0 • >80 % stenosis: EDV > 140 cm/sec
The Doppler Principle f fo skin Velocity Profile v Sample Volume Doppler Measurement of Blood Flow Velocity:
ICA STENOSIS DUPLEX SCAN MRA <50% DR PSV < 125 cm/s ICA/CCA ratio < 2 < 50% DR 50-74% DR PSV > 125 cm/s EDV < 125 cm/s 2 < ICA/CCA ratio < 4 50-74% DR 75-99% DR PSV > 300 cm/s EDV > 125 cm/s ICA/CCA ratio > 4 75-99% DR short (<3 cm) flow gap No ICA flow CCA EDV = 0 Long (>3 cm) flow gap No intracranial ICA signal Criteria of carotid stenosis: Occlusion
Contrast Angiography: High grade ICA stenosis
High Resolution B-mode Imaging: proximal
The ultimate goal of vascular testing is to identify clinically significant carotid disease, so that treatment can be applied and risk of stroke reduced.
Benefit of CEA for Asymptomatic Stenosis: Annual stroke risk Medical tx CEA p value VA 1993 (n=444) 2.4 % 1.2 % > 0.05 ACAS 1995 (n=1662) 2.2 % 1.0 % 0.004
Benefit of CEA for Symptomatic Stenosis: Annual stroke risk Medical tx CEA p value NASCET 1991 > 70 % stenosis 13 % 4.5 % < 0.001 NASCET 1998 50 - 70 % stenosis 4.4 % 3.1 % 0.045
Results of surgery vs. medical therapy: • Absolute Reduction • Symptomatic patients in Stroke Risk • NASCET: > 70% DR 17% @ 2 yr • NASCET: 50-59% 10% @ 5 yr • ECST: > 70% DR 12% @ 3 yr • Asymptomatic patients • ACAS: > 60% DR 6.3% @ 5 yr *multicenter, random assignment - angiography controlled
Cerebrovascular Symptoms Carotid Territory TIA Stroke (-) ECG, CT Scan, MRI/MRA Cerebral Angiography Carotid Duplex Testing >60% ICA Stenosis Isolated Bifurcation Disease Combined Carotid Vertebral–Subclavian Disease Consider for Carotid Endarterectomy ASSESS OPERATIVE RISK Low High Transluminal Angioplasty/Stent
Asymptomatic – Carotid Bruit <60-70% Stenosis >70-80% Stenosis ? Disease Progression ?Contralateral ICA Occlusion Assess life expectancy Assess Operative Risk Medical Treatment • Control of ASO risk factors • Aspirin or Clopidogrel • Surveillance High Risk Good Candidate Isolated Bifurcation Disease Medical Rx, Carotid stent Carotid Endarterectomy
Carotid Endarterectomy: • Considerations: • Anesthesia • General • Regional • Shunt • Patch
Results of Carotid Endarterectomy: Clinical Death/ % of CEAs Series # CEAs Stroke w/o Angio USF 350 0.6%/0.9% 68% Samson 603 0.2%/1.6% 93% Melissano 728 0.4%/1.6% 86% Logason 229 1.2%/2.2% 80% Ascher 903 0.7%/0.7% 94%
Complications: • Cranial nerve injury up to 4-16% • Stroke 1-6% • Hemorrhage/ hematoma 1-5% • Mortality < 1% • Restenosis < 5% (myointimal hyperplasia)
Outcome of Carotid Stent-Assisted Angioplasty versus Open Surgical Repair for Recurrent Carotid Stenosis Andrew N. Bowser, MD Dennis F. Bandyk, MD Avery Evans, MD Michael Novotney, MD Martin R. Back, MD Brad L. Johnson, MD Murray L. Shames, MD Division of Vascular & Endovascular Surgery University of South Florida College of Medicine Tampa, Florida
10-year Concurrent Review (1993-2002) • CAS(1997-2002): 50 patients (52 arteries) • Redo-CEA: 27 patients Re-do CEA CAS Age: 66.5 ± 1170.2 ± 8 p<0.01 Men: 19 (70%) 35 (70%) Co-morbid Conditions: HTN 24 (88%) 44 (88%) p NS CAD 13 (48%) 31 (62%) p NS Smoker 19 (70%) 33 (66%) p NS Lipids 16 (59%) 35 (70%) p NS PVD 12 (24%) 24 (48%) p NS DM 8 (30%) 8 (16%) p = .11
Re-do CEA CAS Number: 27 52 Indication: -Symptomatic 17 (63%) 31 (60%) p NS TIA 4 (15%) 19 (37%) CVA 10 (37%) 7 (13%) p = .02 Both 3 (11%) 5 (10%) -Asymptomatic 10 (37%) 21 (40%) p NS Mean Interval to re-intervention:83 ± 14 mo. 50 ± 8 mo. p < 0.01 Early (<36m) RCS: 10 (37%) 33 (63%) p = 0.03 Nine CAS patients enrolled in Clinical Trials Cordis – Feasibility trial 1 pt. Archer-1(no distal protection) 2 pts Archer-2 (distal protection) 3 pts Crest–Lead-in (distal protection) 3 pts
17 CAS pts not surgical candidates: 33% - Surgically-inaccessible high lesions (n=8) - Severe disabling medical comorbidity (n=4) - Neck irradiation (n=3) - Other (RCS with CN injury) (n=2) • Option of redo-CEA or CAS (n=35) • 3 Redo-CEA Pts Deemed Not CAS Candidates Soft thrombus
30-Day Procedural Outcomes # Transient tongue deviation * Pt treated for combined RCS & MCA stenoses – ICH (day-2) ** all > 24 hrs after CAS procedure
No patient developed ipsilateral stroke Same patient survival @ 36 mo: 92%