Download
1 / 24
240 likes | 696 Views
Irritant dermatitides. Juvenile Plantar- Palmar Dermatosis. AKA sweaty sock syndrome Location Plantar surfaces of feet and big toes, palms Timing Toddlers and school-age Fall or winter Resolution by adolescence Description Chronic, red, scaly patches with fissuring.

E N D
Juvenile Plantar-PalmarDermatosis • AKA sweaty sock syndrome • Location • Plantar surfaces of feet and big toes, palms • Timing • Toddlers and school-age • Fall or winter • Resolution by adolescence • Description • Chronic, red, scaly patches with fissuring
Juvenile Plantar-PalmarDermatosis • Due to wetting of skin during day followed by drying at night • Treatment • Shoes that breathe • Charcoal insoles • Lubrication of feet at night • Topical steroids in severe cases
Irritant dermatitides Lip-licking eczema Thumb sucking eczema
Pityriasisrosea • Benign self-limited disorder • Timing • Most common adolescents and young adults • Prodrome of malaise, h/a • Description • Herald patch • Pink, slightly scaly • May clear centrally
Pityriasisrosea • 5-10 days later • Small lesions: trunk, proximal extremeties • Inverse pityriasis • Lesions predominate on face and distal ext (palms/soles) • Description • Small, round papules • Enlarge to 2mm ovals • Scaly surface • Raised, but can be macular • Erythematous, hyper or hypopigmented • May create “christmas tree” pattern over thorax
Pityriasisrosea • Course • Peaks in several weeks • Duration 2-3 mos • Treatment • No treatment required • Oral erythromycin and UV light may hasten resolution • Etiology unknown • ?infectious?
Keloids • Extend beyond margin of the wound • Most common in Blacks • Treatment • Intralesional steroids • Combination with surgical excision • Often recur
GranulomaAnnulare • Unclear etiology… no treatment required • Annular eruption • Begins as papule that gradually extends peripherally to form a ring • Raised, indurated • Overlying epidermis intact • Same color as adjacent skin • Extensor surfaces • Resolves over months
Categories • Irritant contact derm • Caustic agents (non-allergic) • Allergic contact derm • T-cell mediated (type 4- delayed) • Poison Ivy or Nickel • Initial rxn needs 7-14 day sensitization period • Reexposure provokes rapid rxn (hours)
Rhus Dermatitis (Poison Ivy) • Description • Linear streaks • erythematous papules and vescicles • Large patches (heavy exposure) • Impressive swelling (face, digits, genitalia) • Contact • Sap of plants, objects, smoke • Wash skin immediately • Can not spread after 20min
Photocontact and Phototoxic Reactions • Photocontact (Phototoxic) • True cell-mediated delayed hypersensitivity • Sun exposure precipitates urticarial eruption • Marked by sun exposed areas only • Precipitated by • Tetracycline • Sulfa • Thiazides • NSAIDS • Fluoroquinolones • Griseofulvin • Topical agents
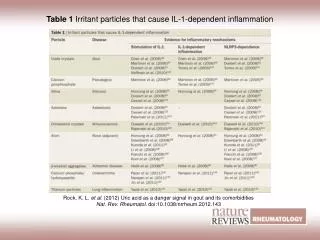
Phototoxins • Agents applied to skin: • Non-immunologic exaggerated sunburn rxn • Photodermatitis most common • Plant-derived photosensitizers: • Psoralens (lemons, limes, figs, dill, parsley, parsnips, carrots, celery) • Macules: Bullae: Hyperpigmented patch • May have bizarre patterns mimicing abuse
Phototoxic Rxn (Psoralens) Lemons Limes Figs Dill Parsley Parsnips Carrots Celery
Treatment of Contact Derm • Localized: topical steroids • Severe or Widespread: systemic steroids • 1mg/kg/day tapered over 2wks • Identification of trigger and avoidance are key!!
Id Reaction • Aka autoeczematization • Widespread secondary eczematous dermatitis • Contact derm • Tinea (particularly at start of therapy)
Classification • Dermatophytes • Tinea (ringworm fungi) • Yeasts • Candida • Diaper dermatitis • Pityrosporum • Tineaversicolor • Both have been implicated in seborrhea
Tineacorporis • Description • Pruritic, annular lesion with central clearing • Border: microvesicles rupture then scale • Acquisition • Direct contact with infected kittens • Trichophytontonsurans • Course • May expand up to 5cm over several weeks
TineaCorporis • Diagnosis • Confirmed by KOH • Loose scales at margin • Long, branching, septate rods of uniform width that cross borders of epidermal cells • Treatment • Glabrous skin areas: topical antifungals • Multiple or widespread: oral griseofulvin
TineaPedis • Aka: Athlete’s foot • Location: • Web spaces b/w toes • Sides of toes • May involve the plantar or dorsal surfaces • Timing: Mostly adolescents • Acquisition: contaminated showers, etc • Warm, moist environments • Description: • Scaling and fissuring • Vesiculopustular lesions and maceration • Intense burning or itching
TineaPedis • Dx: • Clinical grounds • Confirmed by KOH • Tx: • Antifungal creams or powders • Reducing foot moisture • Oral antifungals if severe