Download
1 / 58
770 likes | 2.26k Views
Cell Injury, Cell Death, and Adaptations. Cell adaptation. Hypertrophy Hyperplasia Atrophy Metaplasia. Hypertrophy Vs. Hyperplasia.

E N D
Cell adaptation Hypertrophy Hyperplasia Atrophy Metaplasia
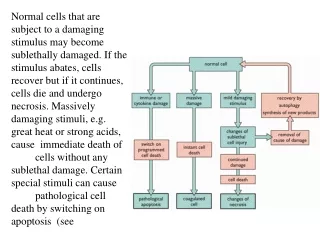
B, Small spindle-shaped uterine smooth muscle cells from a normal uterus. Compare this with (C) large, plump hypertrophied smooth muscle cells from a gravid uterus.
Physiologic hypertrophy of the uterus during pregnancy. A, Gross appearance of a normal uterus (right) and a gravid uterus (left)
This is cardiac hypertrophy involving the left ventricle. The number of myocardial fibers does not increase, but their size can increase in response to an increased workload, leading to the marked thickening of the left ventricle in this patient with systemic hypertension.
Here is one of the nodules of hyperplastic prostate, with many glands along with some intervening stroma. The cells making up the glands are normal in appearance, but there are just too many of them.
The prominent folds of endometrium in this uterus opened to reveal the endometrial cavity are an example of hyperplasia. Cells forming both the endometrial glands and the stroma have increased in number. As a result, the size of the endometrium has increased. This increase is physiologic with a normal menstrual cycle.
The testis at the right has undergone atrophy and is much smaller than the normal testis at the left.
This is cerebral atrophy in a patient with Alzheimer disease. The gyri are narrowed and the intervening sulci widened.
Metaplasia of normal columnar (left) to squamous epithelium (right) in a bronchus, shown (A) schematically and (B) histologically.
Metaplasia of laryngeal respiratory epithelium has occurred here in a smoker. The chronic irritation has led to an exchanging of one type of epithelium (the normal respiratory epithelium at the right) for another (the more resilient squamous epithelium at the left).
Metaplasia of the normal esophageal squamous mucosa has occurred here, with the appearance of gastric type columnar mucosa.
This microscopic appearance of myocardium is a mess because so many cells have died that the tissue is not recognizable. Many nuclei have become pyknotic (shrunken and dark) and have then undergone karorrhexis (fragmentation) and karyolysis (dissolution). The cytoplasm and cell borders are not recognizable.
Here is myocardium in which the cells are dying. The nuclei of the myocardial fibers are being lost. The cytoplasm is losing its structure, because no well-defined cross-striations are seen.
In this example, liver cells are dying individually (arrows) from injury by viral hepatitis. The cells are pink and without nuclei.
In this fetal thymus there is involution of thymic lymphocytes by the mechanism of apoptosis. Individual cells fragment and are consumed by phagocytes to give the appearance of clear spaces filled with cellular debris.
Two large infarctions (areas of coagulative necrosis) are seen in this sectioned spleen. Since the etiology of coagulative necrosis is usually vascular with loss of blood supply, the infarct occurs in a vascular distribution. Thus, infarcts are often wedge-shaped with a base on the organ capsule.
This is an example of coagulative necrosis. This is the typical pattern with ischemia and infarction (loss of blood supply and resultant tissue anoxia). Here, there is a wedge-shaped pale area of coagulative necrosis (infarction) in the renal cortex of the kidney.
Microscopically, the renal cortex has undergone anoxic injury at the left so that the cells appear pale and ghost-like. There is a hemorrhagic zone in the middle where the cells are dying or have not quite died, and then normal renal parenchyma at the far right. This is an example of coagulative necrosis.
The contrast between normal adrenal cortex and the small pale infarct is good. The area just under the capsule is spared because of blood supply from capsular arterial branches. It illustrates the shape and appearance of an ischemic (pale) infarct well.
The liver shows a small abscess here filled with many neutrophils. This abscess is an example of localized liquefactive necrosis.
This is liquefactive necrosis in the brain in a patient who suffered a "stroke" with focal loss of blood supply to a portion of cerebrum. This type of infarction is marked by loss of neurons and neuroglial cells and the formation of a clear space at the center left.
At high magnification, liquefactive necrosis of the brain demonstrates many macrophages at the right which are cleaning up the necrotic cellular debris.
Grossly, the cerebral infarction at the upper left here demonstrates liquefactive necrosis. Eventually, the removal of the dead tissue leaves behind a cavity.
This is fat necrosis of the pancreas. Appear grossly as the soft, chalky white areas seen here on the cut surfaces.
Microscopically, fat necrosis adjacent to pancreas is seen here. There are some remaining steatocytes at the left which are not necrotic. The necrotic fat cells at the right have vague cellular outlines, have lost their peripheral nuclei, and their cytoplasm has become a pink amorphous mass of necrotic material.
This is the gross appearance of caseous necrosis in a hilar lymph node infected with tuberculosis. The node has a cheesy tan to white appearance.
This is more extensive caseous necrosis, with confluent cheesy tan granulomas in the upper portion of this lung in a patient with tuberculosis.
Microscopically, caseous necrosis is characterized by acellular areas, as the tissue architecture is completely lost (at the upper right), surrounded by a granulomatous inflammatory process.
This is gangrene of the lower extremity. In this case the term "wet" gangrene is more applicable because of the liquefactive component from superimposed infection in addition to the coagulative necrosis from loss of blood supply. This patient had diabetes mellitus.
Gangrenous necrosis involves the tissues of a body part. The inflammation seen here is extending beneath the skin of a toe to involve soft tissue (fat and connective tissue) and bone.
Here is fatty change of the liver due to accumulation of lipid in the cytoplasm of hepatocytes.
Here are Mallory bodies (the red globular material) composed of cytoskeletal filaments in liver cells chronically damaged from alcoholism. These are a type of "intermediate" filament between the size of actin (thin) and myosin (thick). (proteins accumulation)
Here are neurofibrillary tangles in neurons of a patient with Alzheimer's disease. The cytoskeletal filaments are grouped together in the elongated tangles.
The yellow-brown granular pigment seen in the hepatocytes here is (lipofuscin) which accumulates over time in cells (particularly liver and heart) as a result of "wear and tear" with aging.