Download
1 / 46
490 likes | 1k Views
DISEASES OF THE PERICARDIUM. H.A.MWAKYOMA, MD. Introduction. The Pericardium is a fibroelastic tissue made up of parietal and visceral layers These two layers are separated by the pericardial cavity

E N D
DISEASES OF THE PERICARDIUM H.A.MWAKYOMA, MD
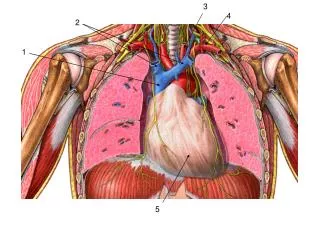
Introduction • The Pericardium is a fibroelastic tissue made up of parietal and visceral layers • These two layers are separated by the pericardial cavity • Pericardial cavity usually contains 15-50 ml of plasma ultrafiltrate in healthy individuals
Diseases of the Pericardium • Pericardial effusion • A. Hemopericardium • B. Cardiac tamponade • 2. Pericarditis • A. Serous D. Hemorrhagic • B. Fibrinous E. Constrictive • C. Purulent
Pericardial Effusion Normal: 15-50 ml of thin serous fluid Sudden increase: up to 200 ml: minimal increase in pressure between 200 and 300 ml: sharp rise in pressure Slow increase: up to 2 liters: minimal increase in pressure
Pericardial Effusion: Common Causes • Viral myopericarditis • Metastatic malignancy • Autoimmune disease • Drug-induced • Renal failure • Bleeding (Hemopericardium)
Pericardial Effusion: Symptoms • Dull constant left chest pain • Dyspnea (shortness of breath) • Less common: • Hiccups (phrenic nerve) • Hoarseness (recurrent laryngeal nerve) • Dysphagia (esophageal compression)
Pericardial Effusion: Signs • Muffled soft heart sounds • Dullness to percussion over lower • posterior left lung (Ewart’s sign) • Decrease in pericardial friction rub
Pericardial Effusion: Diagnosis Chest x-ray: if >250 ml: enlarged globular cardiac silhouette, maybe ECG: decreased voltage, (alternating large and small QRS “electrical alternans” as electrical axis changes as heart swings to and fro in a large effusion, cute but rare)
Pericardial Effusion: Diagnosis Echocardiogram: can provide estimate of size and evidence of tamponade Pericardiocentesis: low yield, best reserved for cases with tamponade when simultaneously diagnostic and therapeutic
Hemopericardium: • Rare, but commonly fatal • Causes: • cardiac rupture after transmural • myocardial infarction (especially day 5), • aortic aneurysm rupture, • chest trauma, • anticoagulation, • leukemia
Cardiac Tamponade: • Pericardial effusion or blood • compressing the heart enough to • impair filling and pumping
Pericardial Tamponade • Increased Pericardial Pressures leading to compression of all cardiac chambers • Pericardial elasticity maybe limited (Acute vs Chronic) • Cardiac chambers become small and chamber diastolic compliance is reduced • Decreased cardiac filling
Cardiac Tamponade: • Symptoms: If sudden: confusion, • agitation, dyspnea, collapse, arrest • If slow: fatigue, leg edema, dyspnea
Cardiac Tamponade: Signs • Jugular venous distention, • muffled heart sounds and • hypotension (Beck’s triad) • Pulsus paradoxus [misnomer]: • exaggeration of normal decrease in blood pressure with inspiration >10 mm Hg systolic • (not specific, also seen in obstructive • airway disease)
Cardiac Tamponade: Diagnosis • Echocardiogram: • diastolic collapse of right atrium and right ventricle • Swan-Ganz right heart catheterization: • increased and equalized right atrial and • left atrial (surrogate: wedge) pressures • Treatment: tap it! (subxiphoid)
PERICARDITIS: • Types of Pericarditis • Serous: smooth surface, scant neutrophils, • lymphocytes and macrophages, usually • with effusion of 50-200 ml of thin fluid • (protein <50% of serum level) • Fibrinous: dry, roughened, shaggy, • “bread and butter” surface, more neutro- • phils, lymphocytes and macrophages, • serofibrinous if with effusion
More Types of Pericarditis • Purulent (synonym: suppurative): red • granular surface coated with pus, lots of • subsurface neutrophils, up to 500 ml • exudate in the pericardium • Hemorrhagic: serous, fibrinous or purulent • plus hemorrhage, +/- effusion or exudate • with blood added • Constrictive: [misnomer] rarely any -itis
Purulent pericarditis is composed of a thin to creamy pus with erythematous, granular serous surfaces
Hemorrhagic pericarditis -This is composed of an exudates of blood admixed with fibrinousto suppurative effusion
chronic constrictivepericarditis the double layered thin pericardial membranes are turned into a single thick, rigid fibrous capsule, which restricts diastolic filling
Acute Pericarditis The most common disease of the pericardium Most common causes 1. Infectious A. Viral (idiopathic) B. Pyogenic bacterial C. Tuberculosis
Viral (Idiopathic) Pericarditis Self-limited, usually over in 1-3 weeks Most common viruses: Coxsackie (especially group B) or echovirus not routinely cultured, so specific diagnosis requires anti-viral titers, acute and convalescent 4-6 weeks later rarely worth doing, so viral pericarditis = idiopathic (sort of, approximately)
Acute Pericarditis: Most common causes 2. Non-Infectious A. Post myocardial infarction B. Metastatic malignancy (lung, breast) C. Autoimmune connective tissue disease D. Drug-induced (e.g. procainamide) E. Radiation-induced F. Renal failure
Acute Pericarditis: Symptoms • Pain: substernal, but sharp, pleuritic • (increased with inspiration), positional • (increased with lying down, decreased • with sitting up and leaning forward) • Dyspnea: not exertional • Fever • (Malaise, myalgias, if viral)
Acute Pericarditis: Physical & ECG signs Pericardial friction rub: evanescent, superficial, scratchy, to and fro, best heard with stethoscope diaphragm, with patient leaning forward, exhaling ECG (abnormal in 90%): ST elevation diffuse (except aVR, V1) with concavity upwards, +/-PR depression
Acute Pericarditis due to Pyogenic Bacteria Pathogenesis: extension of empyema or myocardial abscess OR seeding of pre-existing effusion OR hematogenous infection Evolution: fibrinous adhesions, organization (fibroblasts), fibrous adhesions, “constrictive pericarditis”
Post Myocardial Infarction Pericarditis: • Two Forms • Extension of visceral pericarditis to • parietal over large transmural infarct, • uncommon, <5% of infarctions • 2. Dressler syndrome 2-12 weeks after • infarction, probably autoimmune, • has become rare
Autoimmune Pericarditis: occurs in 30% of patients with lupus (as part of a polyserositis with simultaneous pleuritis and peritonitis), and with rheumatoid arthritis Drug-induced Pericarditis: occurs with procainamide (sometimes as part of a polyserositis), and with hydralazine
Hemorrhagic Pericarditis Rare, associated with 1. metastatic carcinoma 2. leukemia (thrombocytopenia) 3. tuberculosis Skin test for tuberculosis (“PPD”) and chest x-ray: important tests for unexplained pericarditis
Constrictive “Pericarditis” Encasement of the heart in a dense fibrous or fibrocalcific scar which prevents cardiac hypertrophy or dilatation Rare, commonly due to previous purulent or tuberculous pericarditis Pathophysiology similar to tamponade
Constrictive Pericarditis Symptoms: fatigue, leg edema, dyspnea Signs: jugular venous distention (increased with inspiration = Kussmaul’s sign), hepatomegaly, ascites, leg edema
Constrictive Pericarditis ECG: atrial fibrillation (50%), low voltage Chest x-ray: calcification (50%) Cardiac catheterization: dip & plateau right and left ventricular tracings, right atrial prominent y descent
Cardiac Tamponade Jugular venous distention, muffled heart sounds, hypotension, pulsus paradoxus Echocardiogram: diastolic collapse of right atrium and right ventricle Swan-Ganz: equalization of pressures
Acute Pericarditis Most commonly idiopathic (viral), self-limited to 1-3 weeks with Sharp substernal pleuritic positional pain Pericardial friction rub Diffuse upward concavity ST elevation
Examination Question: 1. The pericardial effusion most likely to be fatal is A. Hemorrhagic slowly increased to 1500 ml B. Hemorrhagic suddenly increased to 150 ml C. Serous slowly increased to 2000 ml D. Serous suddenly increased to 100 ml E. Serous suddenly increased to 300 ml
Examination Question • 2. A red granular pericardial surface is • characteristic of • Constrictive pericarditis • Fibrinous pericarditis • Hemorrhagic pericarditis • Purulent pericarditis • Serous pericarditis
Metabolic Disorders • Uremia- • Most common metabolic cause • 6-10 % of ESRD patients not on HD can have Pericarditis • Dialysis related Pericardial Effusions (seen in 13% of patients) • Severe Hypothyroidism • effusion – usually not significant • rarely pericarditis • Ovarian hyperstimulation syndrome • complication of gonadotropin therapy • Due to fluid shifts
Malignancy • Responsible for 6% of acute pericardial disease (pericarditis and tamponade) • Accounts for 15-20% of moderate to large pleural effusions • Mets - Lung, Breast, Hodgkin’s metastases • Primary - Mesotheliomas and lipomas
Collagen Vascular Disease • SLE- pericardial involvement in up to 50% • Rheumatoid Arthritis • Progressive Systemic Sclerosis • MCTD • Polyarteritis • Giant Cell Arteritis • Inflammatory Bowel Disease
Clinical Presentation of Pericarditis • Chest Pain- • sudden onset over anterior chest • sharp and pleuritic • Improves by leaning forward • Radiates commonly to trapezius ridges • Pericardial Friction Rub • ECG – findings depend on stage • 2 of 3 needed to make diagnosis +/- effusion.
Cardiac Biomarkers • Can see elevation in CK, MB, TpnI • 22% of patients with Acute Pericarditis in one trial were above TpnI threshold • Transient rise, resolving within the first 7 days • Patients with higher TpnI did not have higher complication rates
Sinus Tachycardia Elevated JVP Pulsus Paradoxus Rub possible Kussmaul's sign Less likely w/o constrictive component Physical Exam of Tamponade
Pulsus Paradoxus • An exaggerated fall in systemic blood pressure during inspiration • Inspiratory decline in thoracic pressure is transmitted through the pericardium to the right side of the heart • Systemic Venous return increases with inspiration • In tamponade, the rigid pericardium prevents the RV free wall from expanding during diastole causing the pressure transmission to the septal wall and decreased LV filling during inspiration
Acute Pericarditis due to Pyogenic Bacteria Rare, purulent, generally fulminant High mortality Most common BACTERIA: Staphylococcus aureus Streptococcus pneumoniae