Download
1 / 61
620 likes | 848 Views
Overview Of Retinal Conditions Clinical and OCT Findings Central Coast Day Hospital Inaugural Optometrist Conference 26 th February 2012. Anil Arora. What you might rather be doing. What you might feel like right now. 100 Things To Do Before You Die (www.bucketquiz.com).

E N D
Overview Of Retinal ConditionsClinical and OCT FindingsCentral Coast Day HospitalInaugural Optometrist Conference26th February 2012 Anil Arora
100 Things To Do Before You Die (www.bucketquiz.com) • Give your mother a dozen red roses and tell her you love her. • Shower in a waterfall. • Sleep under the stars. • Fart in a crowded space • Give to a charity. • Run a marathon. • Reflect on your greatest weakness, and realize how it is your greatest strength. • Attend a Sunday morning ophthalmology conference in Terrigal -especially any lectures on retinal conditions and OCT
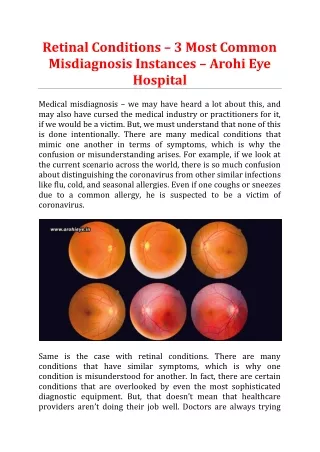
Shows accumulation of fluid within the retina and below the retina Changes in the neurosensory retina Cystic changes Alteration of contour or thickness Vitreous – retinal interface abnormalities Irregularity or elevation of the RPE Quantification of the abnormalities and measurement of treatment response OPTICAL COHERENCE TOMOGRAPHY IN RETINAL DISEASES
Normal macula • Foveal depression • Symmetrical contour • Normal thickness of fovea and perifoveal tissues • Flat and regular RPE
Important Retinal Conditions • Age-related macular degeneration • Diabetic retinopathy • Retinal detachment and predisposing diseases • Central and branch retinal vein occlusion • Macular hole • Epiretinal membrane • Vitreomacular traction syndrome • Central serous retinopathy
Age-Related Macular Degeneration • Leading cause of blindness in the elderly • Prevalence rate rises sharply with each decade • In Australia there are about 5 million people 50+ • ~ 15% of these will have age-related macular changes • 1- 2% or 50-100,000 of these will have significant vision loss from geographic atrophy or from exudative changes
Exudative Macular Degeneration • EXAMINATION • Visual acuity • Variable – depends on size and location of haemorrhage/exudation • Amsler grid testing • Fundus examination • Haemorrhage • Elevation by subretinal fluid/blood • Drusen • Pigment changes/atrophy/scarring
Drusen • Accumulation of debris between the RPE and Bruch’s membrane
Exudative changes –SRF and sub-RPE fluid Fovea SRF RPE SRF and RPE detachment RPE thinned and irregular
Serous PED b PED – serous and fibrovascular dépression fovéale Fovea RD DSR DEP PED Occult Fibro vascular PED
Role of OCT in ARMD • Evaluation of exudative changes • Quantification of retinal thickness • Response to treatment with anti-VEGF agents
Diabetic Retinopathy • Presence of diabetic microvascular lesions • Most frequent ocular complication of DM • 1/3rd rule – About 1/3rd of all diabetics have some degree of retinopathy and in about 1/3rd of these have sight-threatening disease • After 15 years about 70% of people with diabetes will have some retinopathy
Risk Factors For Retinopathy • Development of diabetic retinopathy related to: • Duration of diabetes • Glycaemic control • Hypertension management • Serum lipids and cholesterol • Other factors eg. pregnancy, nephropathy
Diabetic Retinopathy • Two types of retinopathy • Nonproliferative retinopathy (NPDR) • Early stage diabetic retinopathy • Proliferative retinopathy (PDR) • Later stage diabetic retinopathy
Nonproliferative Diabetic Retinopathy (NPDR) • Also called background diabetic retinopathy. • Earliest stage of diabetic retinopathy. • Damaged blood vessels in the retina leak fluid and blood into the eye. • Cholesterol or other fat deposits from blood, called hard exudates, may leak into retina. Top: Healthy retina Bottom: NPDR with hard exudates
Proliferative Diabetic Retinopathy • Characterised by the growth of new blood vessels in response to tissue hypoxia • NVD – new vessels at or within 1 DD of the optic disc • NVE – new vessels elsewhere in the retina • Can lead to: • Vitreous haemorrhage • Tractional retinal detachment
Proliferative Diabetic Retinopathy With PDR, vision is affected when any of the following occur: • Vitreous haemorrhage • Traction retinal detachment • Neovascular glaucoma Vitreous haemorrhage
Diabetic Macular Oedema • Most common cause of decreased vision and blindness in diabetic retinopathy • Indicated by findings of microaneurysms, haemorrhages or hard exudates within 2DD of the fovea • CSME (Clinically significant macular oedema) Complicated definition, but basically retinal thickening or hard exudates within 500 um of the fovea
Macular oedema OCT scan showing macular oedema
Role of OCT in Diabetic Retinopathy • Confirm clinical suspicion of macular oedema • Quantification of extent of oedema • Diagnosis of macular traction and localised macular tractional retinal detachment in cases of proliferative retinopathy • Evaluation of response to treatment – laser and /or intravitreal Avastin/Triamcinolone
Retinal Detachment • Often preceded by a vitreous detachment with patient seeing flashes and floaters • Usually starts as a blurring or loss of peripheral vision in one area that progresses centrally • More likely in those with a history of • Myopia • Ocular trauma or surgery
Retinal Detachment • Most commonly due to a posterior vitreous detachment with a retinal tear developing • About 10% of PVD develop a retinal tear • Risk of tear much higher if blood or pigmented cells present in vitreous
Retinal Detachment • If a retinal tear is found before the retina detaches, it can often be treated with laser photocoagulation or cryotherapy or a combination of these.
Retinal Detachment • Surgical Management • Scleral buckle/cryotherapy • Vitrectomy • +/- buckle/cryotherapy • +/- endolaser • +/- intraocular gas • +/- silicone oil • +/- perfluorocarbon liquid • Pneumatic retinopexy • In-rooms procedure • Gas injection and positioning
Role of OCT in Retinal Detachment • Very limited role as the diagnosis is clinical and treatment in most cases is surgical • Useful in assessing reason for poor vision following retinal detachment repair with anatomical reattachment of the retina. • May show: • Persistent macular oedema/subretinal fluid • Damage to photoreceptors • Thinned and atrophic retina • Epiretinal membrane
Central Retinal Vein Occlusion • Common cause of visual loss • Usually history of hypertension • Two main forms • Non-ischaemic • Ischaemic • 75-80% non-ischaemic at presentation • 15% non-ischaemic may convert to ischaemic • 50% of ischaemic -->neovascular glaucoma
Central Retinal Vein Occlusion Cause Of Visual Loss In CRVO • In non-ischaemic CRVO vision reduction due to macular oedema &/or haemorrhage • In ischaemic CRVO vision reduced from macular ischaemia or later by retinal neovascularization with vitreous haemorrhage or from neovascular glaucoma
Central Retinal Vein Occlusion Management • Macular oedema • Intravitreal Avastin • Intravitreal triamcinolone / dexamethasone • Macular grid laser in younger patients (<60) • Ischaemia and neovascular complications • Panretinal photocoagulation • Anti-VEGF drugs • Management of hypertension and other cardiovascular risk factors
Branch Retinal Vein Occlusion • Usually occurs in patients 50 – 70 yo • Hypertension is the main risk factor (70%) • Occurs at an A-V crossing where vein and artery have a common adventitial sheath • Visual loss from macular oedema, haemorrhage or ischaemia
Branch Retinal Vein Occlusion Late Complications • Retinal or optic disc neovascularization with vitreous haemorrhage • Epiretinal membrane • Chronic macular oedema with formation of a foveal cyst or lamellar hole • “Atrophic maculopathy” from prolonged macular oedema or ischaemia
Branch Retinal Vein Occlusion • Management • Intravitreal Avastin • Intravitreal triamcinolone or dexamethasone • Retinal laser • Manage hypertension and other risk factors
Role of OCT in RVO • Assessment of macular oedema • Quantification of retinal thickness • Response of macular oedema to treatment with intravitreal agents and/or laser • Assessment of late complications – epiretinal membrane, lamellar hole
Macular Hole • Central visual loss in elderly • VA usually 6/36 – 6/60 • 5 – 10% bilateral • Treatment consists of vitrectomy, peeling of the cortical vitreous +/- internal limiting membrane peeling and intravitreal gas injection with one to two weeks of face-down positioning
Macular hole OCT showing a macular hole before and after surgery
Epiretinal Membrane • Usually idiopathic, seen in patients over 60 • Sometimes after vein occlusion, inflammation • Variable effect on vision - blurring, distortion • May have associated cystoid macular oedema • Pseudohole – may look like macular hole • Retinal vessels irregular and tortuous • Vitrectomy and peeling if VA 6/18 or worse or even with better vision but troublesome distortion
Epiretinal membrane Without pseudohole With pseudohole
Role of OCT in Macular Hole and Epiretinal Membrane • Clearly shows hole morphology • Differentiates full-thichness hole from lamellar hole or pseudohole • Demonstrates associated conditions such as macular oedema, macular cyst and vitreoretinal traction • Shows response to treatment eg. closure of macular hole, successful peeling of ERM