Download
1 / 52
580 likes | 1.02k Views
Treatment of Injuries to the Brachial Plexus and Upper Extremity. Andrew I. Elkwood , MD, FACS Plastic & Reconstructive Surgery Director, The Center for Treatment of Paralysis and Reconstructive Nerve Surgery. Rehabilitative Surgery.

E N D
Treatment of Injuries to the Brachial Plexus and Upper Extremity Andrew I. Elkwood, MD, FACS Plastic & Reconstructive Surgery Director, The Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Rehabilitative Surgery Patients with disabilities can do more with less (depending upon the quality of their rehabilitation treatment) Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Nerve Surgery The “Garage Door” Analogy Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Nerve Surgery • The “Garage Door” Analogy • Outlet = spinal cord • Wire = nerve • Motor = muscle • Chair = tendon • Door = hand or foot Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Rehabilitative Surgery is a process not an event Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Rehabilitative SurgerySurgical Algorithm Nerve Repair Nerve Grafting Neurotization Tendon Transfer Tenodesis Joint Fusion Splinting Elegance Simplicity Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Nerve Grafting • Self transfer (i.e. Sural Nerve) • Manufactured Nerve • Processed Nerve • Cadaver Transplant • Living Related Transplant Center for Treatment of Paralysis and Reconstructive Nerve Surgery
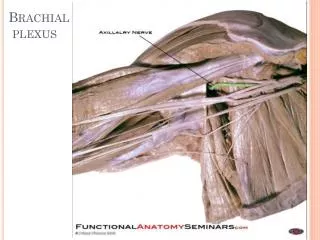
IN THE AREA OF THE PLEXUS • NERVES • BONES • ARTERY • VEIN • LUNG Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Center for Treatment of Paralysis and Reconstructive Nerve Surgery
BRACHIAL PLEXUS INJURIES • BIRTH INJURY • MOTOR VEHICLE ACCIDENTS • MOTORCYCLES • FALLS • INDUSTRIAL ACCIDENTS • SPORTS INJURIES • TUMORS • RADIATION Center for Treatment of Paralysis and Reconstructive Nerve Surgery
BRACHIAL PLEXUS INJURIES • 4% OF ALL MOTORCYCLE ACCIDENTS • 19% ARE COMATOSE • 13% HAVE C-SPINE INJURIES Center for Treatment of Paralysis and Reconstructive Nerve Surgery
THREE BASIC FACTORS • PAIN • SENSIBILITY • MOTION Center for Treatment of Paralysis and Reconstructive Nerve Surgery
OVERVIEW • DIAGNOSIS • WORK-UP • NERVE STUDIES • NERVE REPAIR • POST-OP • REHABILITATION Center for Treatment of Paralysis and Reconstructive Nerve Surgery
DIAGNOSIS • Often clouded by coma, etc • Often clouded by orthopedic injuries • Often ignored • Often misinformed • May be subtle Center for Treatment of Paralysis and Reconstructive Nerve Surgery
WORK UP • PRELIMINARY WORK UP OF NERVE STUDIES STARTS RIGHT AWAY • FIRST EMG AT 6 WEEK TO 3 MONTHS • CXR • MRI • CT MYELOGRAM Center for Treatment of Paralysis and Reconstructive Nerve Surgery
WORK UP • REPEAT EMG AT 6 MONTHS IF NO IMPROVEMENT • IF IMPROVEMENT REASSESS AT 9 MONTHS • IF NO IMPROVEMENT OPERATE Center for Treatment of Paralysis and Reconstructive Nerve Surgery
TIMING • THE TEXTBOOKS ARE WRONG • DO NOT WAIT A YEAR • IF NOT IMPROVED BY 3 MONTHS, THEY WILL NOT IMPROVE • EMG AT 6-8 WEEKS • REPAIR AT ABOUT 3 MONTHS • ALLOWS FOR “SECOND SHOT” BEFORE ONE YEAR Center for Treatment of Paralysis and Reconstructive Nerve Surgery
SURGERYTEAM APPROACH • SURGEONS • CONSULTANTS • NURSES • THERAPISTS • HOME CARE • FAMILY Center for Treatment of Paralysis and Reconstructive Nerve Surgery
RECOVERY • WHEN NERVE REPAIR IS REQUIRED, RECOVERY IS DELAYED • 1 - 2 MONTH LATENCY • NERVE GROWTH • 1 mm/day • 1 inch/month • LONGER DISTANCE, LONGER RECOVERY TIME Center for Treatment of Paralysis and Reconstructive Nerve Surgery
POST-OP CARE • UNDERLYING DISEASE • MULTIPLE OPERATIONS • PAIN RESISTANCE • SEVERAL OPERATIVE SITES • IMMOBILIZATION • LONG PROCEDURES • ANESTHESIA TIME Center for Treatment of Paralysis and Reconstructive Nerve Surgery
REHABILITATION • IMMOBILIZATION • 3 - 6 WEEKS POST-OP • AGGRESSIVE REHAB • KEEP JOINTS SUPPLE • MAINTAIN STRENGTH • BUILD NEW STRENGTH • RELEARN MUSCLE MOVEMENT • BIOFEEDBACK Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Spinal Accessory Neurotization Brachial Plexus Palsy Center for Treatment of Paralysis and Reconstructive Nerve Surgery
BRACHIAL PLEXUS PALSY Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Nerve Transplants • Its all about spare parts • No need to prioritize • Can’t go to home depot • Cadaver • Living related donor Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Nerve Transplant • NO NEED TO PRIORITIZE • NO NEED TO PRIORITIZE • NO NEED TO PRIORITIZE • NO NEED TO PRIORITIZE Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Nerve Transplantation • Allograft • Abo Compatibility • Prograf • Wrist Monitoring • Steroid Rescue Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Nerve Transplantation • Who’s a candidate? • Injury about 1 year • Good health • Good support system • Massive injury Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Nerve Transplantation • Who’s a good donor? • Good health • Abo match • No communicable disease Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Nerve Transplantation CADAVER VS. LIVING RELATED DONOR Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Spinal Cord Injury Can we treat spinal cord injuries like bilateral brachial plexus injuries? Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Spinal Cord Injury Tetraplegic Hand Surgery Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Spinal Cord InjuryHand Surgery • Minimize Spasticity • Maximize passive range of motion • Maximize active range of motion • Tendon Lengthening • Joint Stabilization/Joint Fusion • Splinting Static/Dynamic • Tendon Transfer/ Tenodesis Effect • Neurotization Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Spinal Cord Paralysis We can’t fix the problem but we can help to RESTORE FUNCTION Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Spinal Cord Injury • Need for Functioning Donors • Nerve donors above the lesion • Muscle donors for tendon transfers • Free muscle donors • Sacrifice contra lateral side? Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Spinal Cord Paralysis • Level of Injury • Cranial nerves always spared • Cervical plexus always spared Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Spinal Cord Paralysis • Prioritize Function • Arm Abduction • Triceps • Bicep • Wrist Extension • Finger Extension/Flexion • Individualize for Patient Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Spinal Cord Injury Timing • Need to let injury evolve • Need to maximize therapy • Need to maintain existing function • Motor end plates do not degrade • Spasm must be balanced • Can take advantage of two-stage procedures Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Spinal Cord Injury • Trapezius to Deltoid Transfer • Neurotization from spinal accessory nerve • Nerve to levator scapulae • Nerve to sternocleidomastoid • Latissmmus to bicep • Latissimus to triceps Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Stroke Why can’t we treat a stroke patient like a brachial plexus patient? • Medical problems • Spasm Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Spinal Cord InjuryPressure Sores • Can occur over any bony prominence • Sacrum most common • Scalp • Ischium • Hip • Heels Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Spinal Cord InjuryPressure Sores • Prevention • Prevention • Prevention • Prevention • Prevention • Prevention • Prevention Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Spinal Cord InjuryPressure Sores • Any pressure above capillary perfusion pressure is to high • Only a Clinitron works to heal a wound • Other mattresses may work to help prevent • Floating the pressure point is best • Extra padding is bad • Prevention is HARD work Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Spinal Cord Injury Treatment of Pressure Sores • Grading scale has no value • Maximize inflow • Maximize protoplasm • Remove “bacteria food” • Means of debridement is not of great importance • Re-educate patient • The VAC does not debride Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Spinal Cord InjuryPressure Sore Treatment • High recurrence rate • Maximize everything • Quality of soft tissue coverage • Bed trial • Social support • Prognosis Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Spinal Cord InjuryPressure Sores • Prevention • Prevention • Prevention • Prevention • Prevention • Prevention • Prevention Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Spinal Cord InjuryPressure Sores • Neurotization for protective sensibility Center for Treatment of Paralysis and Reconstructive Nerve Surgery
Spinal Cord InjurySummary • We do not have a cure • We have treatments to deal with complications • We have cutting edge methods to maximize function and impact lives • Education is our greatest hurdle Center for Treatment of Paralysis and Reconstructive Nerve Surgery