Download
1 / 38
380 likes | 635 Views
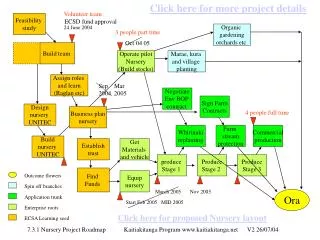
Animal model to study feasibility of VV ECMO using RRT platform – Pilot study. Abhay Divekar, MD, FRCPC, FSCAI Director Pediatric Cardiac Catheterization Laboratory University of Iowa Children’s Hospital Iowa City, IA. Health Sciences Center, Winnipeg, Manitoba. Alex Gutsol, MD.

E N D
Animal model to study feasibility of VV ECMO using RRT platform – Pilot study Abhay Divekar, MD, FRCPC, FSCAI Director Pediatric Cardiac Catheterization Laboratory University of Iowa Children’s Hospital Iowa City, IA Health Sciences Center, Winnipeg, Manitoba Alex Gutsol, MD Todd Koga, RTR Gale Bonin, RN Helen Cooper, RN
All clinical and research activities performed at the University of Manitoba, Winnipeg, Canada Disclosure – Gambro Canada Provided a Prismaflex Unit for experimental use
Continuous Renal Replacement Therapy Improvised to Provide Extracorporeal Membrane Oxygenation A Divekar1, R Soni1, M Seshia2,T Drews3, M Kesselman3, G Bonin4, C Press4, M Maas5, J Minski6, T Blydt-Hansen7. Cardiology1, Neonatology2, Critical Care3, Clinical Nurse Specialist CRRT Program4, Cardiac Perfusion5, Respiratory Therapy6, Nephrology7, Department of Pediatrics Health Sciences Center, Winnipeg, Manitoba, Canada Full term infant needing VV-ECMO for severe PPHN secondary to MAS After all ECMO is just a pump and a membrane ! Background FiO2 100%, PaO2 25-40, PaCO2 60-80, OI 40-80 Inotropic support, “resuscitation” - Dopamine 10 mcg/kg/min epinephrine 1.0 mcg/kg/min FiO2 100%, PaO2 80-90, PaCO2 50-60, OI 15; but poor systemic oxygen delivery, lactate 10, poor urine output Oxy – CRRT - FiO2 40-50%, PaO2 50-70, PaCO2 35-55, OI <15, Lactate 2 Dopamine off, Epinephrine 0.2 mcg/kg/min
RRT platforms have been successfully used for other indications • Severe sepsis and septic shock • Removal of “evil humors” • Molecular Adsorbent Recirculating System – MARS • Extracorporeal liver replacement • ARDS, pulmonary edema
Do we need an oxygenating RRT platform when ECMO exits? Are there any potential applications?
Patients requiring CRRT – not needing full ECMO support • s/p cardiac surgery – AKI – fluid retention • pulmonary edema • RRT increasingly used • ? Reduce ventilator needs and avoid iatrogenic injury • Rescue situations ?? • “Developing countries” - ? Simpler ECMO
Validation of the system – pilot study • Animal model • Adapting RRT platform for oxygenation • Circuit • Catheters • Oxygenator • Alarms
Animal Model • All animal work performed in accordance to CCAC and University Animal Care Committee guidelines • Domestic Farm Swine 2 - 9 kg (n = 6) and one 50 kg blood donor • First three animals • Cannulation technique • Access and return via same vessel vs. separate vessels • Catheter size and placement • Circuit preparation • Need to add mannitol • Absolute need for heater-cooler exchanger • Need to normalize prime • Older animals tolerate acute hypoxemic respiratory failure poorly and therefore need to be place on support rapidly
Animal Model • Three animals weighing 2.4, 2.8 and 5.5 kg formed the experimental cohort • Induction and maintenance anesthesia - isoflurane in oxygen • Intubated and mechanically ventilated • achieve normal arterial blood gas • Continuous EKG, invasive arterial pressure, systemic saturation, core temperature
Animal Model • Femoral vessels and external jugular vessels were isolated by surgical cutdown • Femoral arterial line • Largest possible double lumen cannula (7-12 Fr) for return line – femoral vein • Largest possible double lumen cannula (7-12 Fr) for access – external jugular vein
Animal Model • Unfractionated heparin sulfate 300 U/kg given after isolating the vessels • ACT maintained at 180-220 secs with additional heparin boluses
Animal Model • Acute respiratory failure induced by hypoventilation and normobaric hypoxia (10% FiO2 – blending in nitrous oxide, oxygen and medical air) • Arterial blood gas obtained to demonstrate respiratory failure
Priming the CRRT circuit • Prismaflex – Gambro – RRT platform • Flow rate up to 450 ml/min • Pre-packaged ST-100 filter – loaded through automated steps • Primed with 1000 ml NS with 5000 unit of heparin • CVVHDF mode • Pre blood pump prime with Prismasol4 solution (100 %) pre-filter • Dialysate solution Prismasol4
Priming Lilliput 2 (D902) hollow fiber oxygenator • PVC ¼” tubing - venous inlet and arterial outlet • Primed and de-aired with normal saline • AV loop clamped and ¼ x ¼ inch Cobe connector (M–F) – spliced in-line • Heater-cooler exchanger
Splicing the hollow fiber oxygenatorin the return linepre-air detection filter
After splicing oxygenator in-line • Blood prime - Donor blood collected and stored in ACD blood bags from a 50 kg swine • Pigs have weak blood group antigens do not need cross match • no lawyers either ! • Add mannitol to blood bag (1 g/kg) • Sweep flow 1 lit, 100% FiO2 • Normalize prime (pre-blood pump replacement solution and dialysate solution) – 30 min BFR 100 ml/min, PBP – 500 ml/min, Dialysate 500 ml/min
Initiation of VV - ECMO • Start at 75 ml/min and increase by 50 ml/min • Maximum flow of 400 ml/min • Limiting access/return line/filter pressure • Obtain ABG, pre and post oxygenator blood gas analysis • Record all monitored and software calculated pressures • Record all alarms
Sat Sat PaCO2 Sat PaCO2 PaO2 PaO2 PaO2 PaCO2
7 Fr 7 Fr 7 Fr 7 Fr 7 Fr 7 Fr
Results • Animal model of acute hypoxemic respiratory failure useful to study and adapt RRT platform for VV ECMO • Very efficient at CO2 removal • With adequate flow rates can support veno-venous membrane oxygenation • Minimal recirculation with access from external jugular vein and return via the femoral vessels • Circuit resistance (tubing size, stop-cocks, filter) and catheter size major limitation to flow
Limitations of experimental setup • Pilot project – limited number of animals • Only short term (hours) data available • Longer term data in terms of filter clotting/change needed • Limited cannula choice • Hemolysis not evaluated • Sweep flow and % FiO2 not adjusted • Only one type of oxygenator evaluated • Anemia
Limitation if the modification is used with the circuit as is • Circuit shutdown for malfunction and warning alarms • 72 hours mandatory filter change • Tubing/circuit resistance
Future Work • Circuit design • Minimize sites of resistance, ? Large tubing size • Optimal filter • High flow stopcock • Access and return cannula • novel design with DL cannula • femoral cannulation in small infants may compromise venous drainage and therefore have limited clinical application • Optimal oxygenator • Prevent automatic clamping of the return line for malfunction and warning alarms • Study a larger group of animals in each group and for a longer duration
Acknowledgements • The Winnipeg Rh Institute Foundation • Gambro Canada • Sorin Medical • Section of Pediatric Nephrology, Health Sciences Center, Winnipeg, Manitoba
Results Baseline ARF Flow 83 ml/kg/min Flow 133 ml/kg/min
Results Baseline ARF Flow 71 ml/kg/min Flow 125 ml/kg/min
Results Baseline ARF Flow 45 ml/kg/min Flow 56 ml/kg/min