Download
1 / 41
430 likes | 847 Views
Acute leukemia. Mohammed Al-matrafi . Leukemia. Malignancy of leucocytes precursors Appearance of abnormal cells in BM, peripheral blood, infiltration in LN, Liver spleen etc. Childhood Leukemia. Types: Based on clinical presentation Acute leukemia 95% Chronic leukemia 5%

E N D
Acute leukemia Mohammed Al-matrafi
Leukemia • Malignancy of leucocytes precursors • Appearance of abnormal cells in BM, peripheral blood, infiltration in LN, Liver spleen etc.
Childhood Leukemia Types: Based on clinical presentation • Acute leukemia 95% • Chronic leukemia 5% Based on type of predominant leukemic cells • Acute leukemia: Acute lymphoblastic leukemia- 85% Acute myeloid leukemia- 15%
Childhood leukemia Prevalence: • Most common malignancy in children • 30% of all pediatric malignancies • Average incidence 4/100,000 children • Peak age: ALL : 4 years AML: Same from birth –10 years
Etiology Unknown: Genetic predisposition Viral infection Cong. immune deficiency Ionizing radiation Certain toxic chemicals
Genetics • At risk: Trisomy 21 {15 times} Fanconi aplastic anemia Ataxia telengectasia Siblings of patient with ALL {2-3 times} Identical twins{ concordance of ALL}
Clinical presentation ofALL • SYMPTOMS: Usually < 4 weeks history at diagnosis Fatigue/malaise Fever/infection Extremity, joint or bone pain Bleeding manifestations CNS symptoms (Increased ICP) Weight loss Others: DIC, Chloroma {AML}
Clinical Presentation of ALL • SIGNS: Pallor Hepatomegaly Spleenomegaly Lymphadenopathy Petechie Bony tenderness
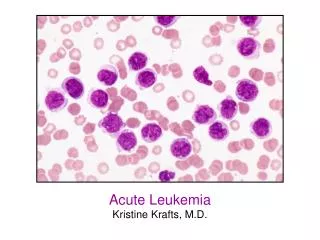
Diagnosis • Peripheral blood : CBC : Normal, increased, decreased > 100,000 bad prognosis Anemia Neutropenia Blast cells Thrombocytopenia
L1 L2 L3
:Diagnosis • Bone marrow (BM) Morphology: >25% blast cells in marrow (normal <5%)
Other investigations • Uric acid high • LDH high
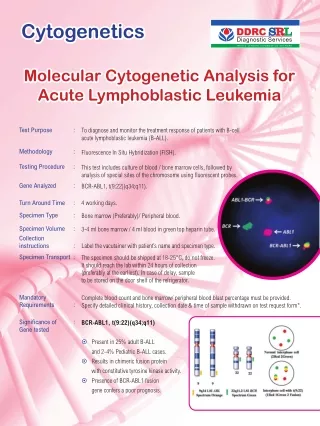
Bone marrow aspirate • Morphological classification: • Cytochemical analysis: • Immune phenotyping: • Cytogenetic: • Molecular studies:
Morphology • FAB classification: { depending on size,cytoplasm,nucleus} L1 L2 L3 L1: commonest and has good prognosis
Immune phenotype • T cell leukemia • B cell leukemia • Non T cell non B cell leukemia
Cytogenetic studies • Higher ploidy { >50 chromosomes}: good prognosis • Diploidy or hyperdiploidy: { 47-50 chromosomes} Intermediate prognosis • Haploid cell: worst prognosis
Differential diagnosis Non malignant conditions like: • Juvenile Rheumatoid Arthritis / other connective disorders • Infectious Mononucleosis • Aplastic Anemia • Idiopathic Thrombocytopenic Purpura {ITP}
Treatment of ALL BASED ON: • Lineage (B or T) • Cytogenetic abnormalities • Patient’s age and other risk factors • White blood cell count (WBC)
Supportive measures • Hydration • Treatment of infection • Correction of electrolyte disturbances • Blood product transfusion • Psychological support • Treatment of tumor lysis syndrome
Treatment of ALL REQUIRES: • Intensive systemic multi agent chemotherapy • Repetitive intrathecal chemotherapy • Cranial irradiation when necessary in older children • Bone marrow transplant in special circumstances • Treatment continued for 3 years
Treatment • Induction phase: 4 weeks {3-4 drugs} vincristine, prednisilone, L-asparaginase etc • CNS prophylaxis: Intrathecal methotrexate Cranial irradiation • Consolidation phase:2-4 weeks {For prevention of relapse} • Maintenance phase:{2-5 years}
Sanctuaries areas • Relatively impermeable to the medications: • Sites of relapse: 2 sites: CNS Testis
Prognostic factors {contd.} • Morphology, histochemistry, cytogenetic L1; good prognosis • Response to induction therapy Rapid- good prognosis Slow- poor prognosis • B cell leukemia: worst prognosis
Prognostic factors • Demographic Age: <2year,>10year poor prognosis Race: Black poor prognosis Sex: Male poor prognosis • Leukemic burden WBC: >50,000 poor prognosis Mediastinal LN: poor prognosis CNS involvement. at diagnosis: poor prognosis
Outcome • Relapse sites: Bone marrow CNS Testis in males • Disease free for 5 years after diagnosis: overall 60-70%, in standard risk group 80% • Relapse: Allogenic bone marrow transplant
Bone marrow transplant • Very high risk cases • Following relapse
Bone marrow transplantBlood stem cell transplant • Autologous • Allogeinic
In a blood stem cell transplant, the patient is first given a pre-transplant treatment of chemotherapy and/or radiation therapy to destroy the patient's leukemia cells and immune system. Blood stem cells are then put into the patient's blood to restore the patient's immune system and blood production.
Acute myelogenous leukemia • FAB classification: M1,M2,M3,M4,M5,M6,M7 M3 { promyelocytic} may present with DIC • Disease free survival with chemotherapy 30 % BMT 50-60 %
Questions • Commonest childhood malignancy • Types of Ac leukemia • Peak age • Etiology • At risk Patients • Symptoms • Signs • Diagnosis: PBS and bone marrow changes • D/D • Sanctuary areas • Prognostic factors: eg: age <1year,female ,white races ,WBC > 100,000, mediatinal mass, CNS invol L1 type , Rapid response to induction therapy • Relapse site • BMT indication