Download
1 / 1
20 likes | 329 Views
Acceptance and Commitment Therapy as an Alternative to Exposure: A Pilot Study in the Treatment of Veterans Diagnosed with PTSD Katharine C. Sears, Ph.D. 1,2 ; Varvara Mazina, B.A. 1,2 ; Amy Wagner, Ph.D. 3 ; Robyn D. Walser, Ph.D. 1

E N D
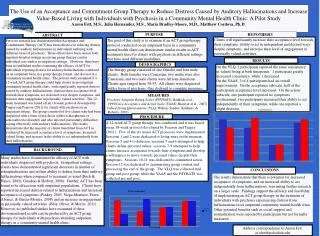
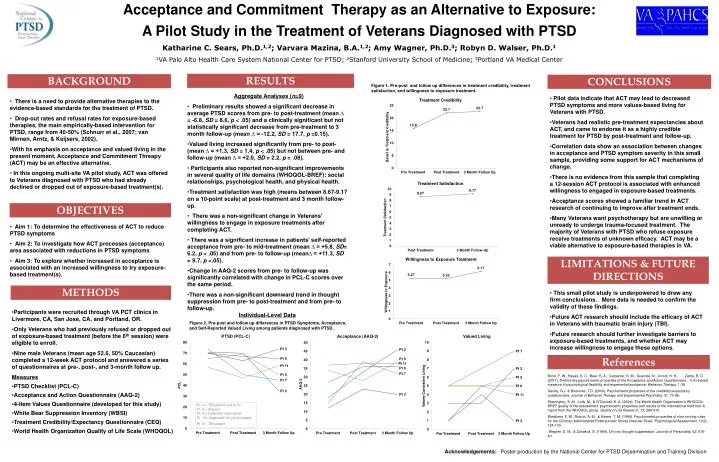
Acceptance and Commitment Therapy as an Alternative to Exposure: A Pilot Study in the Treatment of Veterans Diagnosed with PTSD Katharine C. Sears, Ph.D.1,2; Varvara Mazina, B.A.1,2; Amy Wagner, Ph.D.3; Robyn D. Walser, Ph.D.1 1VA Palo Alto Health Care System National Center for PTSD; 2Stanford University School of Medicine; 3Portland VA Medical Center RESULTS BACKGROUND CONCLUSIONS Figure 1. Pre-post and follow up differences in treatment credibility, treatment satisfaction, and willingness to exposure treatment. • Aggregate Analyses (n=9) • Preliminary results showed a significant decrease in average PTSD scores from pre- to post-treatment (mean ∆ = -6.8, SD = 8.6, p < .05) and a clinically significant but not statistically significant decrease from pre-treatment to 3 month follow-up (mean ∆ = -12.2, SD = 17.7, p =0.15). • Valued living increased significantly from pre- to post- (mean ∆ = +1.3, SD = 1.4, p < .05) but not between pre- and follow-up (mean ∆ = +2.0, SD = 2.2, p = .08). • Participants also reported non-significant improvements in several quality of life domains (WHOQOL-BREF): social relationships, psychological health, and physical health. • Treatment satisfaction was high (means between 8.67-9.17 on a 10-point scale) at post-treatment and 3 month follow-up. • There was a non-significant change in Veterans' willingness to engage in exposure treatments after completing ACT. • There was a significant increase in patients’ self-reported acceptance from pre- to mid-treatment (mean ∆ = +5.8, SD= 6.2, p < .05) and from pre- to follow-up (mean∆ = +11.3, SD = 9.7, p <.05). • Change in AAQ-2 scores from pre- to follow-up was significantly correlated with change in PCL-C scores over the same period. • There was a non-significant downward trend in thought suppression from pre- to post-treatment and from pre- to follow-up. • Individual-Level Data • Pilot data indicate that ACT may lead to decreased PTSD symptoms and more values-based living for Veterans with PTSD. • Veterans had realistic pre-treatment expectancies about ACT, and came to endorse it as a highly credible treatment for PTSD by post-treatment and follow-up. • Correlation data show an association between changes in acceptance and PTSD symptom severity in this small sample, providing some support for ACT mechanisms of change. • There is no evidence from this sample that completing a 12-session ACT protocol is associated with enhanced willingness to engaged in exposure-based treatments. • Acceptance scores showed a familiar trend in ACT research of continuing to improve after treatment ends. • Many Veterans want psychotherapy but are unwilling or unready to undergo trauma-focused treatment. The majority of Veterans with PTSD who refuse exposure receive treatments of unknown efficacy. ACT may be a viable alternative to exposure-based therapies in VA. • There is a need to provide alternative therapies to the evidence-based standards for the treatment of PTSD. • Drop-out rates and refusal rates for exposure-based therapies, the main empirically-based intervention for PTSD, range from 40-50% (Schnurr et al., 2007; van Minnen, Arntz, & Keijsers, 2002). • With its emphasis on acceptance and valued living in the present moment, Acceptance and Commitment Threapy (ACT) may be an effective alternative. • In this ongoing multi-site VA pilot study, ACT was offered to Veterans diagnosed with PTSD who had already declined or dropped out of exposure-based treatment(s). OBJECTIVES • Aim 1: To determine the effectiveness of ACT to reduce PTSD symptoms • Aim 2: To investigate how ACT processes (acceptance) area associated with reductions in PTSD symptoms • Aim 3: To explore whether increased in acceptance is associated with an increased willingness to try exposure-based treatment(s). LIMITATIONS & FUTURE DIRECTIONS Figure 2. Pre-post and follow up differences in PTSD Symptoms, Acceptance, and Self-Reported Valued Living among patients diagnosed with PTSD. METHODS • This small pilot study is underpowered to draw any firm conclusions. More data is needed to confirm the validity of these findings. • Future ACT research should include the efficacy of ACT in Veterans with traumatic brain injury (TBI). • Future research should further investigate barriers to exposure-based treatments, and whether ACT may increase willingness to engage these options. • Participants were recruited through VA PCT clinics in Livermore, CA, San Jose, CA, and Portland, OR. • Only Veterans who had previously refused or dropped out of exposure-based treatment (before the 6th session) were eligible to enroll. • Nine male Veterans (mean age 52.6, 50% Caucasian) completed a 12-week ACT protocol and answered a series of questionnaires at pre-, post-, and 3-month follow up. • Measures • PTSD Checklist (PCL-C) • Acceptance and Action Questionnaire (AAQ-2) • 4-Item Values Questionnaire (developed for this study) • White Bear Suppression Inventory (WBSI) • Treatment Credibility/Expectancy Questionnaire (CEQ) • World Health Organization Quality of Life Scale (WHOQOL) References Bond, F. W., Hayes, S. C., Baer, R. A., Carpenter, K. M., Guenole, N., Orcutt, H. K., . . . Zettle, R. D. (2011). Preliminary psychometric properties of the Acceptance and Action Questionniare - II: A revised measure of psychological flexibility and experiential avoidance. Behavior Therapy, 1-38. Devilly, G.J. & Borkovec, T.D. (2000). Psychometric properties of the credibility/expectancy questionnaire. Journal of Behavior Therapy and Experimental Psychiatry, 31, 73-86. Skevington, S. M., Lotfy, M., & O'Connell, K. A. (2004). The World Health Organization's WHOQOL-BREF quality of life assessment: psychometric properties and results of the international field trial. A report from the WHOQOL group. Quality of Life Research, 13, 299-310. Weathers, F. W., Ruscio, A. M., & Keane, T. M. (1999). Psychometric properties of nine scoring rules for the Clinician-Administered Posttraumatic Stress Disorder Scale. Psychological Assessment, 11(2), 124-133. Wegner, D. M., & Zanakos, S. (1994). Chronic thought suppression. Journal of Personality, 62, 616-40. Pt. 1 = TBI patient lost to f/u Pt. 4 = dropout Pt. 8 = treatment interruption Pt. 10= treatment not yet complete Pt. 3 = TBI patient Acknowledgements:Poster production by the National Center for PTSD Dissemination and Training Division