Download
1 / 28
360 likes | 498 Views
Carbapenemase - Producing Carbapenem -Resistant Enterobacteriaceae. Nicole Hearon, HAI Epidemiologist Surveillance and Investigation Division Indiana State Department of Health. Objectives. At the end of the presentation attendees should be able to:

E N D
Carbapenemase-Producing Carbapenem-Resistant Enterobacteriaceae Nicole Hearon, HAI Epidemiologist Surveillance and Investigation Division Indiana State Department of Health
Objectives • At the end of the presentation attendees should be able to: • Understand and describe the basic epidemiology of carbapenemase-producing carbapenem-resistant Enterobacteriaceae (CP-CRE) • Report cases of CP-CRE via I-NEDSS • Determine appropriate and efficient interventions that can prevent CP-CRE transmission in healthcare settings
Definitions • Enterobacteriaceae: a family of bacteria normally found in human intestines; can become carbapenem-resistant; can cause serious infection when spread outside the gut • Carbapenem: a class of broad-spectrum antibiotics used to treat severe infections; antibiotics of last resort when other antibiotics are not available (e.g., imipenem, meropenem, doripenem, ertapenem) • Carbapenemase: enzymes that break down (inactivate) carbapenem antibiotics, causing resistance • CRE: a family of germs that are difficult to treat because they are highly resistant to antibiotics
CP-CRE Definition • Organisms that are non-susceptible to at least one carbapenem antibiotic with MIC ≥ 2 µg/ml or zone diameter ≤ 22 mm (≤ 21 mm for ertapenem) AND • Meet one of the following criteria:(next slide)
CP-CRE Definition (cont’d) • Positive for carbapenemase production by a phenotypic test (e.g., Modified Hodge or Carba NP) OR B. Nonsusceptible to at least three (3) carbapenem antibiotics with MIC ≥ 2 µg/ml or zone diameter ≤ 22 mm (≤ 21 mm for ertapenem)OR C. Positive for a carbapenemase gene marker • Examples: Klebsiella pneumoniae carbapenemase (KPC), New Delhi Metallo-beta lactamase (NDM), Verona Integron-Encoded Metallo-beta-lactamase (VIM), Oxacillinase-48 (OXA-48), Imipenemase Metallo-beta-lactamase (IMP)
Why are CRE epidemiologically important? • Cause infections with high mortality rates (up to 50%) • Carry genes with high levels of resistance to many antimicrobials, limiting treatment options • Resistance can be transmitted between organisms or between patients • Spread rapidly and require the most rigorous infection control measures • Have spread throughout many areas of the U.S. and can spread more widely
Carbapenem Resistance • Enterobacteriaceae can become resistant to carbapenems by: • The transmission of resistance genes from one bacterium to another • The production of enzymes that inactivate carbapenems (i.e., carbapenemases)
Transmission • Person to person • via contact with infected or colonized individuals • via hands of healthcare personnel • via contaminated medical equipment • Contact with stool or wounds • Contact with contaminated environmental surfaces (e.g., bed rails)
States with CP-CRE in 2006 https://www.ihaconnect.org/Quality-Patient-Safety/Documents/Webinars/CfC-cre-webinar-presentation-2014-09-25-final.pdf
Current States with CP-CRE http://www.cdc.gov/hai/organisms/cre/TrackingCRE.html
Global Dissemination of CRE Molton J, et al. Clin Infect Dis 2013;56:1310-1318 http://cid.oxfordjournals.org/content/56/9/1310.full?sid=b2bcabcc-cb4d-41ab-ba19-b91734089663
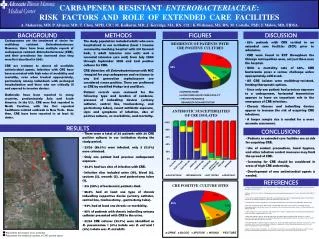
Risk Factors • Exposure to acute care or long-term care facilities • Exposure to an ICU • Presence of other medical conditions • Compromised immune system • Invasive devices (e.g., ventilators, central venous catheters, or urinary catheters) • Invasive procedures (e.g., endoscopic procedures) • History of extensive antibiotic use
Types of Infections • CP-CRE can cause: • Bloodstream infections • Ventilator-associated pneumonia • Surgical site infections • Intra-abdominal abscesses • Urinary tract infections
Detection • Appropriate specimens: • Stool • Blood • Urine • Wound • Laboratory tests: • Modified Hodge Test • Carba NP (CarbapenemaseNordmann-Poirel) • Polymerase chain reaction (PCR) • – Sputum • – Bile
Treatment • Colonized patients • No antibiotics needed • Infected patients • Antibiotics are limited • Other therapies (e.g., draining the infection) • Strains that have been resistant to all antibiotics have been reported
Infection Control Measures • When CP-CRE are identified: • An investigation shall be performed by the local health officer within seventy-two (72) hours and include individuals who have shared a residence with the patient in an acute care or long term care facility. • The facility should initiate Contact Precautions;additional precautions should be added if any other transmissible condition is present.
Infection Control Measures (cont’d) • Supplemental measures for a healthcare facility with CP-CRE transmission include the following: • Refer to the most recent CRE Toolkit from CDC at http://www.cdc.gov/HAI/organisms/cre/ • Consider screening patients to determine if they are epidemiologically linked • Consider chlorhexidine gluconate bathing • Case definition is established by the department.
Reporting • CP-CRE must be reported to the health department within 72 hours • IP can create a communicable disease report (CDR) • Select “Carbapenemase producing – Carbapenem resistant Enterobacteriaceae (CP-CRE)” from the drop down list • ISDH HAI Epidemiologist will assign CDR to the LHD
Reporting (cont’d) • Electronic lab reports (ELRs) are also be submitted to ISDH via I-NEDSS by laboratories • ISDH HAI Epidemiologist will assign ELR to LHD • Laboratories must submit isolates within 3 business days of isolation • Only submit one isolate per patient
Investigation • LHD contacts facility IP within 72 hours of notification • Ensure facility places patient on Contact Precautions • Determine if patient has shared a room or staff with other patients • Determine if there is a potential for transmission within facility
Investigation (cont’d) • Local health departments should also: • Promote antimicrobial stewardship • Ensure facility communicates patient’s infection/colonization status to receiving facility (e.g., LTC facility) if patient will be transferred • Inter-facility transfer form with laboratory reports • Complete case investigation in I-NEDSS
Inter-facility Transfer • If a CP-CRE patient will be transferred to a different facility: • Infection Preventionist or designee should notify the accepting facility AND send an “inter-facility infection control transfer form” which should include: • Patient name, date of birth, medical record number • Sending facility contact information • Type of isolation precautions for patient • Infection, colonization, or history of positive culture of a multidrug-resistant organism • Symptoms • Antibiotic use, vaccines • Contact information for person completing transfer form http://www.cdc.gov/HAI/toolkits/InterfacilityTransferCommunicationForm11-2010.pdf
Prevention Recommendations • Healthcare personnel should: • Practice hand hygiene • Clean & disinfect patient rooms and medical equipment • Don PPE before entering patient room • Doff PPE and wash hands before exiting patient room • Keep colonized or infected patient in a single room on Contact Precautions • Dedicate equipment and staff • Only prescribe antibiotics when necessary • Remove temporary medical devices
Patient Screening • Point prevalence surveys: • Used to quickly evaluate the prevalence of CP-CRE in specific wards/units • Screen all patients in a specific high-risk ward/unit • Could be conducted once or multiple times (e.g., if colonization is more widespread or during an intervention) • Screening of epidemiologically linked patients: • Screen contacts of patients to identify transmission • Contacts: • Roommates of CP-CRE patients or patients who may have been cared for by the same healthcare personnel http://www.cdc.gov/hai/pdfs/cre/CRE-guidance-508.pdf
References • http://www.cdc.gov/hai/organisms/cre/index.html • http://www.cdc.gov/hai/organisms/cre/TrackingCRE.html • http://www.cdc.gov/hai/pdfs/cre/CRE-guidance-508.pdf • http://phil.cdc.gov/phil/home.asp • http://ce.nurse.com/RVignette.aspx?TopicId=8822 • http://www.cdc.gov/vitalsigns/hai/cre/infographic.html • https://www.ihaconnect.org/Quality-Patient-Safety/Documents/Webinars/CfC-cre-webinar-presentation-2014-09-25-final.pdf • https://www.youtube.com/watch?v=-FfMCv8FUXI&feature=youtu.be • https://www.youtube.com/watch?v=vnAtuG9ULB4 • http://www.cdc.gov/nhsn/PDFs/pscManual/2PSC_IdentifyingHAIs_NHSNcurrent.pdf • http://www.cdc.gov/drugresistance/threat-report-2013/pdf/ar-threats-2013-508.pdf#page=53 • http://www.fda.gov/MedicalDevices/Safety/AlertsandNotices/ucm434871.htm • http://www.mayoclinic.org/ercp-procedure/IMG-20007655 • http://www.cdc.gov/drugresistance/threat-report-2013/pdf/ar-threats-2013-508.pdf#page=11
Questions or Remarks? Email: nhearon@isdh.in.gov