Download
1 / 20
210 likes | 618 Views
A Patient in Labor with Marfan Syndrome. Aubrey Ballard, SRNA Missouri State University. Objectives . Presentation of Case Study Marfan Syndrome Marfan Syndrome and Pregnancy Marfan Syndrome and Anesthesia Answer Questions. Patient Information. 20-something year old, female

E N D
A Patient in Labor with Marfan Syndrome Aubrey Ballard, SRNA Missouri State University
Objectives • Presentation of Case Study • Marfan Syndrome • Marfan Syndrome and Pregnancy • Marfan Syndrome and Anesthesia • Answer Questions
Patient Information • 20-something year old, female • Transported via EMS in labor, 175/115 • Limited prenatal care; preeclampsia • History of methamphetamine use (quite 4 months prior). Negative urine drug screen • “Writhing in pain”, noncompliant with instructions, not allowing monitoring or additional lab work • Anesthesia consulted for labor epidural
Patient Information • Allergies: Codeine • Current medications: multi-vitamin, magnesium gtt • Anesthesia interview conducted
Marfan Syndrome (MFS) • Autosomal dominate genetic defect in fibrillin-1 or fibrillin-2 gene • Fibrillin is a major component of microfibrils and also help store TGF-β • Inherited or de novo germline mutations • Diagnosis made from physical features & heredity
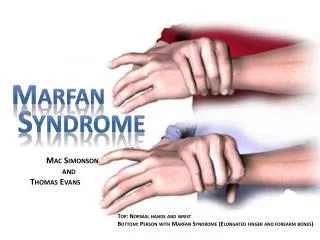
Changes associated with MFS • Cardiovascular • Aortic dilation/dissection – especially at the root • Aortic and mitral valve prolapse/regurgitation • Pulmonary artery dilation • Arrhythmias, cardiomyopathy, congestive heart failure • Skeletal • Arachnodactyly with hyperextensibility • Chest wall deformities • Scoliosis/kyphosis • Osteoporosis • High arched pallet, retrognathia, micrognathia
Changes associated with MFS • Ocular • Lens subluxation • Myopia • Cataracts • Retinal detachment • Glaucoma • Pneumothorax/pulmonary blebs, asthma, emphysema • Inguinal and incisional hernias • Dilation of dural sac • Dissection of cranial arteries and aneurysmal subarachnoid hemorrhage
Marfan & Pregnancy • Pregnancy increases the likelihood of cardiovascular complications in patients with MFS • Approximately 15% of MFS patients develop a major CV manifestation with pregnancy & 40% have obstetric complications • Prophylactic treatment with beta-blockers or internal defibrillators has been suggested before conception • Increased CO during labor and after delivery increases risk of aortic rupture • Vaginal delivery vs. Cesarean section • Prolonged maternal bleeding
Marfan & Anesthesia • In depth history and physical • Hemodynamic management of cardiovascular conditions; Arterial line • General vs regional (no epinephrine for blocks) • Possible difficult intubation; minimize laryngoscopic response • Careful positioning – joint laxity • Dural ectasia • Recognize and treat aortic dissection
S/S of Aortic Dissection • Important to distinguish dissection from ischemia • Abrupt onset of severe chest or back pain • Does not respond to nitrates or beta-blockers acutely but may decreased with decrease in blood pressure • New aortic diasolic murmur, unequal peripheral pulses or BP, absence of rales with chest pain • Ischemia may occur with aortic root involvement
Treatment of dissection • Lowering BP & decreasing myocardial contractility • X-ray, echo, MRI, CT, TEE • Anticoagulation/thrombolytic therapy contraindicated • Need for surgery based on size and location • MFS aneurysm >4.5 cm indicates need for operative repair
Case Study • Emergent Cesarean Section with RSI • In room at 0936 with BP – 155/105 • Incision at 0943 with deliver of baby at 0944 • BP decreased to 92/68 • Extubated without difficulty and transported to PACU • CT
CT findings • A dissection that starts in the distal aortic arch between the takeoff of the left subclavian and the aberrant right subclavian artery that extends throughout the thoracic aorta, ending just above the level of the celiac trunk and upper abdominal aorta. The takeoff of the aberrant right subclavian artery is ectatic measuring 2 cm in diameter. The distal aortic arch is ectatic measuring 3.2 cm in diameter.
Case Study • Taken to ICU • Cardiology consult • Received 2 units PRBC for H&H of 8.1/24 • Next day was transferred to larger facility
References • Elisha, S. (2011). Aortic Dissection. Case Studies in Nurse Anesthesia. 282-285. • Nagelhout, J.J., Plaus, K.L. & Rieker, M. (2014). Respiratory, Anatomy, Physiology, Pathophysiology & Anesthetic Management. Nurse Anesthesia. 653 • Kasper, Dennis L. (2005). Harrison's Principles of Internal Medicine. Revised/Expanded ed. New York: McGraw-Hill, Medical Pub. Division.2329-2330 • Andropoulos, D., Stephen S., Isobel R., and EmadM. (2010). Anesthesia for Congenital Heart Disease. 2nd ed. Oxford: Blackwell. • Coté and Lerman's a Practice of Anesthesia for Infants and Children. Revised/Expanded ed. Philadelphia, PA: Elsevier/Saunders, 2013. • Bongard, F.S., and Darryl Y.S. (2008) Current Diagnosis & Treatment Critical Care. Revised/Expanded ed. New York: McGraw-Hill Medical.
References • Hall, J. (2005). Principles of critical care (Revised/Expanded ed.). New York: McGraw-Hill, Medical Pub. Division. • Tintinalli, J. (2011). Tintinalli's emergency medicine: A comprehensive study guide (Revised/Expanded ed.). New York: McGraw-Hill. • Marfan Foundation. (2013). What is Marfan Syndrome. Retrieved August 19, 2014, from http://www.marfan.org/about/marfan • FBN1 gene. (2014, August 12).Genetics Home Refernce. Retrieved August 17, 2014, from http://ghr.nlm.nih.gov/gene/FBN1 • Goland, S., & Elkayam, U. (2009). Cardiovascular Problems in Pregnant Women With Marfan Syndrome. Circulation, 619-623.
References • Hanumanthaiah, D. & Sudhir, V. (2013). Neuraxial block in a patient with duralectasia. Indian Journal of Anaesthesia. 624-625 • Bagirzadeh, L., Guglielminotti, J. & Loeys, B. (2013). Anesthesia recommendations for patients suffering from Marfan syndrome. Orphan Anesthesia. 2-8.