Download

1 / 23
230 likes | 376 Views
STRATEGIES FOR OFFERING LONG ACTING METHODS. Reproductive Health / Family Planning Symposium Sept 19-20, 2011 Amman- Jordan ENRIQUITO LU, MD. MPH RH/FP/Cervical Cancer Prevention Unit Technical Director Jhpiego /Baltimore. Session Outline. Situational Summary of Key I ndicators

E N D
STRATEGIES FOR OFFERING LONG ACTING METHODS Reproductive Health/ Family Planning Symposium Sept 19-20, 2011 Amman- Jordan ENRIQUITO LU, MD. MPH RH/FP/Cervical Cancer Prevention Unit Technical Director Jhpiego/Baltimore
Session Outline • Situational Summary of Key Indicators • Jordanian MWRA characteristics • Unmet Needs • Long-Acting Methods and Injectables (LAMI) • What are they? • Why are they essential? • Issues and Challenges • Selected opportunities for expanding LAMI • Summary
Jordan and its MWRA • Population of 6.6 m • 1.6 m MWRA (est) • TFR 3.8 • 1:3 with parity > 5 • Urban Dwellers 4:5 • Method Type • Modern – 41 % • Traditional – 15 % • FP Source – 2:3 private • 4 Primary Reasons not using • Fertility Related -2/3 • Method Related-1/4 • Opposition to Use – 6% • No Knowledge – 0.3 %
UNMET FP NEEDS Demand for FP to: • Limit • Urban – 7 % • Rural – 7 % • Space • Urban – 5 % • Rural – 7 %
IMPACT OF LAMI ON CPR:USING CYPs Couple Years Protection • Estimated protection during a one-year period • Estimates coverage and allows comparison of FP methods coverage • 4 DMPA injections for 1 CYP versus 2.0 CYP for every Implanon Implant http://www.usaid.gov/our_work/global_health/pop/techareas/cyp.html, 2009
Long-acting and Permanent Methods of ContraceptionLA/PM • Long-Acting Methods • IUD • Implants • Permanent Methods • Bilateral Tubal Ligation • Vasectomy (NSV) • Most effective – > 99 % • Safe • Convenient – 1 action = years of effective protection
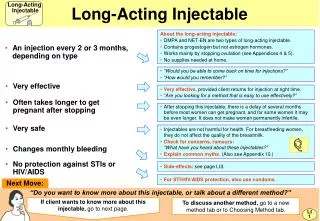
Female sterilization Vasectomy IMPORTANT!Only condoms protect against both pregnancy and STIs/HIV/AIDS SAFETY & EFFECTIVENESS: FP METHODS Most effective and nothing to remember. Very effective but must be carefully used. Effective but must be carefully used. Fewer side-effects, permanent: Fewer side-effects: Fewer side-effects: LAM Male and female condom Vaginal methods Fertility awareness-based methods More side-effects: More side-effects: IUD Implants Pills Injectables Decision Making Tool (adapted), WHO, 2005
LAMI and MWRA Reproductive Intentions IUDs Implants D H Limiting births after desired fertility goals are reached S L Delaying first births -Youth HIV+ can use any LAM Spacing between births -Postpartum -Postabortion Figure Adapted from Bakamjian, ESD 2010
BARRIERS TO LAMI ENVIRONMENTAL • Social-cultural norms, gender issues • Misconceptions and Myths HEALTH SYSTEMS • Policy and Guidelines • Access, commodities, supply PROVIDER/FACILITY • Bias, scheduling,provider type • Knowledge and skills CLIENT • Lack of awareness, cost • Side effects and complications LACK OF ACCESS IS POSSIBLY THE PRIMARY BARRIER
STRATEGIES FOR LAMI • Advocacy at all levels • Work with communities to address barriers, including gender norms • Focus on essentials of service delivery: access, choice, safety and quality • No missed opportunities: - postpartum, postabortion, interval - static and mobile outreach - private and public • Ensure contraceptive security New Mother in Albania (photo credit G. Stolarsky)
US Nurse Practitioner - SOP • Diagnosing and managing acute/chronic diseases • Ordering and doing diagnostic studies • Prescribing physical/rehabilitation treatments • Prescribing drugs for acute and chronic illness Providing • prenatal and family planning services • Well-child care • Primary and specialty care services, health-maintenance care for adults, including annual physicals • Care for patients in acute and critical care settings • Performing minor surgeries and procedures • Counseling and educating patients
TASK SHARING FOR EXPANDING ACCESS • Task sharing - allowing appropriately trained health workers with less formal medical education to deliver the same services as those with more education, where appropriate. • Global Examples of Task sharing • Nurses/midwives in HIC inserting IUDs, implants • Midwives in Indonesia inserting Implants • Surgical nurses in Thailand performing postpartum TL • CHW provision of DMPA (> 12 countries) FP SERVICES
Issues in implementing task shifting • Overloading - always seem to shift to the same cadres • Inadequate support for those “receiving” new tasks • Incentives/motivation/salaries • Making it easy to progress through levels • Educational system that permits re-entry • Competencies described at all levels • Having a clinical career ladder • Need buy-in from professional association • Dealing with regulation of practice
Why Community Based FP Provision? • Expanded points of service are critical for progress • Close the gap on providers shortage • Diminish issues with long distances/wait time at overburdened facilities • Evidence shows community provision increases FP uptake • Essential to reach underserved peri-urban urbanand rural population
CHW AND INJECTABLES: POLICY RECOMMENDATIONS Overall conclusions and policy implications: • Trained CHWs can initiate and reinject DMPA • CHW expands choice and access for underserved and increases uptake • Sufficient evidence exists for national policies to support introduction, continuation, and scale-up Programmatic guidance: • Monitoring and supervision of CHW is needed • Auto-disable syringes should be used • WHO guidance should be followed regarding eligibility WHO,USAID,FHI, Technial Consultation, 2009
Key approaches for Community Access to FP • Trained midlevel (nurses/midwives) and community health worker provision of FP services such as including injectables, implants and IUDs. • Outreach or mobile clinics/teams to provide FP particularly LAMs - implants • Increased access to FP services at clinics and outposts • Pharmacy/drug shop sales and provision of FP methods including injectables
PPFP/PA FAMILY PLANNING ISSUES • Generally, FP is not being provided to amenorrheic women • Providers have misconceptions about fertility return and often make assumptions about sexual activity- limits service access • Challenges for counseling-based methods- LAM takes time • Contact with women limited; providers are busy; Need to provide additional staff for FP when integrated in larger, busy clinics
PPFP BestPractices: Global Experience • Offering FP information and services immediately postpartum and at multiple points during maternal care. • Initiating LAM-very effective method for up to six months; LAM users transition to other methods. • Providing a variety of contraceptive options including short and long acting methods. • Attention to postpartum long-acting and permanent methods. • Integrating PPFP into mother and child care—such as immunizations. Women waiting outside for services Photo credit: Barbara Deller
FP/RH Package Provided by MNH CHW: Bangla Desh P-value: <0.05 Contraceptive Use at 3,6,12 mos PP 41% of women at 12 month postpartum used any modern method in intervention arm compared to 25% in comparison arm
Gender Approached to Reduce Unintended Pregnancies • Encouraging male partners to take more responsibility • Encouragement of joint decision-making and shared responsibility for FP • Institutionalization of gender into both private and public sector RH services, including accreditation • Advocacy with religious leaders and policymakers • Integration with development activities (water and sanitation) • Use of established male networks to diffuse information, refer to services and expand method choice • Empowering female providers IGWG, SUMMARY REPORT, 2011
GENDER INTEGRATION: RH OUTCOMES • Greater contraceptive knowledge and approval; • Increases in positive attitudes toward contraceptive methods; • Increased communication between partners or couples about health; • Longer birth spacing; • Increased use of long-acting contraceptive methods; • Increased health-provider knowledge of family planning; and • Improved quality of care in health facilities. IGWG, SUMMARY REPORT, 2011
TAKE HOME MESSAGE • LAMI have high potential to: • Correct the method skew • Fulfill unmet need for contraception • Revitalize stagnating CPR • Lessons from other countries opens up opportunities for increasing access to LAMI: • Task shifting • Community base approaches • Incorporating Gender Based Approaches • Maximizing utilization of PPFP