Download
1 / 11
110 likes | 311 Views
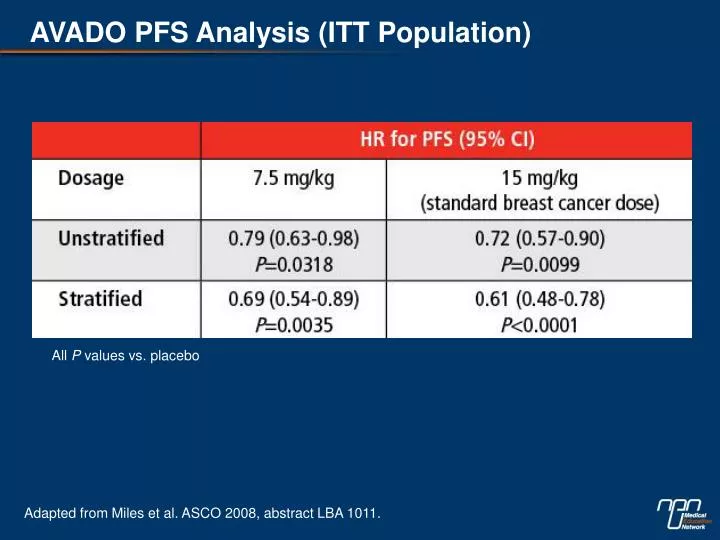
AVADO PFS Analysis (ITT Population). All P values vs. placebo. Adapted from Miles et al. ASCO 2008, abstract LBA 1011. AVADO: Response (patients with measurable disease), %. † mg/kg q3w. Adapted from Miles et al. ASCO 2008, abstract LBA 1011. E2100 and AVADO Serious Adverse Events (%).

E N D
AVADO PFS Analysis (ITT Population) All P values vs. placebo Adapted from Miles et al. ASCO 2008, abstract LBA 1011.
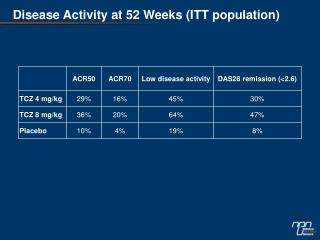
AVADO: Response (patients with measurable disease), % †mg/kg q3w Adapted from Miles et al. ASCO 2008, abstract LBA 1011.
E2100 and AVADO Serious Adverse Events (%) *ATE: arterial thromboembolic events. No increase in venous thromboembolic events was observed with bevacizumab in either study • Adapted from Miller et al. N Engl J Med 2007;357-2666-76. • Adapted from Miles et al. ASCO 2008, abstract LBA 1011.
Primary end point: progression-free survival (PFS) Secondary end points: overall response rate, overall survival, quality of life E2100 Study Design: Randomized, double-blind, placebo-controlled, multicentre, phase III trial Paclitaxel 90 mg/m2 qw for 3 weeks of a 4-week cycle (n=354) Progressive disease (PD)* Previously untreated MBC (n=722) *No crossover permitted Paclitaxel + bevacizumab 10 mg/kg q2w (n=368) PD Adapted from Miller et al. N Engl J Med 2007;357:2666-76.
E2100 Trial: PFS Results Paclitaxel/bevacizumab: 11.4 months 1.0 Paclitaxel: 6.11 months 0.8 HR=0.51 (0.43-0.62) Log rank test P<0.0001 0.6 PFS proportion 0.4 0.2 6.11 11.4 0.0 0 6 12 18 24 30 Months 484 events reported (89% of required events) Adapted fromMiller et al. N Engl J Med 2007;357:2666-76.
E2100 Trial: Overall Response Rate Paclitaxel Paclitaxel/bevacizumab P<0.0001 P<0.0001 40 37.7 29.9 30 Overall response rate (%) 20 16.0 13.8 10 339 341 262 236 0 All patients Measurable disease Adapted from Miller et al. N Engl J Med 2007;357:2666-76.
AVADO Study Design: Randomized, double-blind, placebo-controlled, multicentre, phase III trial Docetaxel 100 mg/m2 q3w + placebo PD All patients were given the option to receive bevacizumab with second line chemotherapy Previously untreated MBC (n=705) Docetaxel + bevacizumab 7.5 mg/kg q3w PD Docetaxel + bevacizumab 15 mg/kg q3w PD Docetaxel was administered for a maximum of nine cycles but earlier discontinuation was permitted Primary end point: PFS Secondary end points: overall response rate, duration of response, time to treatment failure, overall survival, safety and quality of life Adapted from Miles et al. ASCO 2008, abstract LBA1011.
AVADO: Response (patients with measurable disease), % Adapted from Miles et al. ASCO 2008, abstract LBA1011.
AVADO: Safety Summary Adapted from Miles et al. ASCO 2008, abstract LBA1011.
AVADO: Grade ≥3 Adverse Events of Special Interest,* % Adapted from Miles et al. ASCO 2008, abstract LBA1011.
Ongoing RIBBON 1 Phase IIITrial Study Design Chemotherapy† + bevacizumabi.v. 15mg/kg q3w or 10 mg/kg q2w Chemotherapy* + bevacizumab i.v. 15mg/kg q3w PD Previously untreated MBC (n=950), 2:1 Randomization Chemotherapy* + placebo (i.v. on day 1 of 21-day cycle) Chemotherapy† + crossover to bevacizumab 15mg/kg q3w or 10 mg/kg q2w PD Anthracycline-based combination chemotherapy, Q3w taxane (docetaxel or protein-bound paclitaxel) or capecitabine as determined by investigator prior to randomization †Chemotherapy regimen at investigator discretion Primary end point: hierarchical PFS Adapted from Albain K. ASCO 2008.