Download
1 / 107
1.13k likes | 1.4k Views
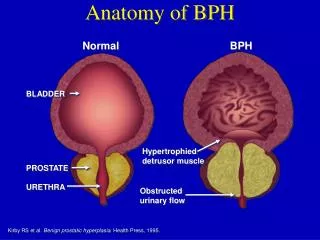
BPH. Benign Prostatic Hyperplasia. PROSTATE GLAND. a walnut-sized gland found in the true pelvis of males just behind the symphysis pubis. composed of several regions or lobes that are enclosed by an outer layer of tissue (capsule) Three distinct zones: peripheral zone (PZ)

E N D
PROSTATE GLAND • a walnut-sized gland found in the true pelvis of males just behind the symphysis pubis. • composed of several regions or lobes that are enclosed by an outer layer of tissue (capsule) • Three distinct zones: • peripheral zone (PZ) • central zone (CZ) • transitional zone (TZ)
PROSTATE GLAND • Benign prostatic hyperplasia uniformly arise in the transitional zone • 60-70% of carcinomas originate in the peripheral zone • 10-20% in the TZ • 5-10% in the CZ
Benign Prostatic Hyperplasia • Characterized by hyperplasia of prostatic stromal and epithelial cells, resulting in the formation of large, fairly discrete nodules in the periurethral region of prostate • With sufficient growth the nodules can compress the urethral canal causing partial, or sometimes complete obstruction of urethra inhibiting urine flow • Not considered as a premalignant tumor [ PSA]
Incidence & Epidemiology • Most common benign tumor in men • Incidence is age-related • 20% - men aged 41-50 • 50% - men aged 51-60 • 90% - men older than 80
ETIOLOGY • Risk factors are poorly understood [multifactorial] • BPH involves both the stromal and epithelial elements of the prostate undergoing hyperplastic changes • Seems strongly tied to endocrine control [levels of free testosterone and estrogen] • As men age the androgen receptors of the prostate becomes increasingly sensitive/hormonally dependent on testosterone and dihydrotestosterone (DHT) production
Dihydrotestosterone (DHT) • In both cell types (stroma/epithelial), DHT binds to nuclear androgen receptors and signals the transcription of growth factors that are mitogenic • Though testosterone can also bind to androgen receptors and cause growth stimulation, DHT is 10x more potent because it dissociates from androgen receptors more slowly
PATHOLOGY • BPH originates from the transition zone • Hyperplastic process resulting from increase number of cells
PATHOLOGY • Nodular growth pattern composed of stroma and epithelium • BPH nodules in the transition zone enlarge and compress the outer zones of the prostate formation of surgical capsule
PATHOPHYSIOLOGY • Symptoms are either obstructive or secondary response of the bladder to the outlet resistance • As enlargement ensues, mechanical obstruction may result from intrusion into the uretheral lumen or bladder neck high bladder outlet resistance
PATHOPHYSIOLOGY • Stroma composed of smooth mm and collagen is rich in adrenergic nerve supply autonomic stimulation sets a tone to the prostatic urethra • Irritative voiding complaints are secondary response of the bladder to increased outlet resistance
Symptoms • Obstructive • Hesitancy • Force and caliber of stream • Sensation of incomplete bladder emptying • Double voiding • Straining to urinate • Post-void dribbling • Irritative • Urgency • Frequency • Nocturia
Symptoms • AUA (American Urological Association) Symptom Score questionnaire • Single most important tool to evaluate patients with BPH • Recommended for all patients before initiating therapy • Self-administered • Identifies the need to treat • Monitors therapeutic response • Scoring: 0-35
Source: Smith’s General Urology, 17th ed.
Signs • Physical examination • DRE • Focused neurologic examination
Signs • Size and consistency • Smooth, firm, elastic enlargement of the prostate=BPH • Induration=CA? • Further evaluation: PSA, transrectal US, biopsy
Laboratory Findings • Assessment of renal function • Urinalysis • Serum creatinine • Renal insufficiency: • 10% of patients with prostatismupper-tract imaging • Risk of postoperative complications from surgical intervention for BPH • Serum PSA: Optional
Imaging • Upper-tract imaging (intravenous pyelogram or renal US) • Recommended only in the presence of concomitant urinary tract disease or complications from BPH
Cystoscopy • Not recommended to determine need for treatment • Assist choosing surgical approach for invasive therapy
Additional Tests • Cystometrograms and urodynamic profiles • Tests for bladder capacity & pressure, and lower urinary tract symptoms (bladder, urethra) respectively • Suspected neurologic disease • Failed prostate surgery • Flow rate measurement, post-void residual urine, pressure-flow studies • Optional
Differential Diagnosis: • Urethral Stricture • Bladder Neck Obstruction • hx of previous urethral instrumentation, urethritis or trauma • Bladder Stones- Hematuria and pain • UTI- Mimics the irritative symptoms of BPH • Urinalysis and culture • Neurogenic Bladder- hx of neurologic problems, stroke, dm, or back injury. • PE: diminished perineal or lower extremity sensation or alteration in bulbocavernous reflex
Treatment: • Mild symptoms (score 0-7)- watchful waiting • Surgical indications • refractory urinary retention • recurrent UTI • recurrent gross hematuria • bladder stones • renal insufficiency • large bladder diverticula
Medical Therapy: • Alpha blockers • alpha-1-adrenoreceptors located in the prostate and bladder • Contractile response of prostate to agonists • Selective blockade of α1a receptors = fewer A.E. • 5α-reductase inhibitors (Finasteride) • blocks conversion of testosterone to dihydrotestosterone • ↓ size of prostate • Improvement of symptoms (>40cm)
Medical Therapy: • Combination therapy • Alpha blockers + 5α-reductase inhibitors • Phytotherapy • use of plants or plant extracts for medicinal purposes • MOA, efficacy and safety unknown
Conventional Surgical Therapy: • Transurethral resection of the prostate (TURP) • Done endoscopically • Symptom score and flow rate improvement • Longer hospital stay • TUR syndrome • Transurethral incision of the prostate • More rapid less morbid • Open Simple Prostatectomy • Done when the prostate is too large to be removed endoscopically
Conventional Surgical Therapy: • Open Simple Prostatectomy • Glands >100g • With concomitant bladder diverticulum or bladder stone or dorsal lithotomy position is not possible
Conventional Surgical Therapy: • Simple Suprapubic Prostatectomy • Procedure of choice in dealing with concomitant bladder pathology • Simple Retropubic Prostatectomy • The bladder is not entered
Minimally Invasive Therapy: • Laser Therapy • Transurethral Electrovaporization of the Prostate • Hyperthermia • Transurethral Needle Ablation of the Prostate • High Intensity Focused Ultrasound • Intraurethral Stents • Transurethral Balloon • Dilation of the Prostate
Prostate Cancer Prostate Cancer • most common cancer diagnosed & is the 2nd leading cause of cancer death in American men • Incidence continues to with advancing age (no peak) • Lifetime risk of a 50-yr old man for latent CaP: 40%; clinically apparent: 9.5%; death from CaP: 2.9%
Risk factors: • Increasing age • Race • Family history • High dietary fat intake • Exposure to chemicals (e.g. cadmium)
Molecular genetics • Chromosome 1 • Gene responsible for familial prostatic cancer • Tumor suppressor genes (8p, 10q, 13q, 16q, 17p, 18q) • Found in the regions human genome
Pathology • Nature : • More than 95% are adenocarcinomas • 5% are transitional cell carcinomas • 90% are neuroendocrine (“small cell”) carcinomas or sarcomas
Histologic characteristics • - hyperchromatic, enlarged nuclei, w/ prominenent nucleoli • - cytoplasm abundant & slightly blue-tinged or basophilic • - absent basal cell layer • - HMW keratin immunohistochemical staining
Origin of Prostatic cancer • Peripheral zone- 70% • Transitional zone- 10 to 20% • Central zone- 5 to 10%
Prostatic Intraepithelial Neoplasia (PIN) • - Precursor to invasive prostatic cancer • - Basal cell layer of the glandular architecture is present • Classifications: • High grade PIN • - associated with invasive Prostatic cancer in 50-80% of cases • Low grade PIN • - ~20% of the cases
Prostatic Intraepithelial Neoplasia (PIN) classic histologic features: - intermediate-to-large size preexisting glands displaying nuclear and nucleolar enlargement and fragmented basal cell layer
Grading and Staging • Gleason score or Gleason sum • primary grade + secondary grade • Gleason grades: 1- 5 • Gleason scores: 2 - 10 • Tumor Grade Score • Well-differentiated 2 - 4 • Moderately-differentiated 5 - 6 • Poorly-differentiated 8-10
Gleason grades 1 & 2 • - small, uniformly shaped glands, closely packed, w/ little infiltrating stroma
Gleason 1 • The most important difference between Gleason pattern 1 and 2 is the presence or absence of circumscription
Gleason 2 • The glands are round to oval and uniformly placed. There are no sharply-angulated or distorted glands.
Gleason 3 • - Variable-sized glands that percolate between normal stroma • Cribriform pattern • - a small mass of cells is perforated by several gland lumens w/ no intervening stroma cookie-cutter-like appearance of cell nests • - smooth border
This example of Gleason grade 3 cancer shows abundant amphophilic cytoplasm, enlarged nuclei with prominent nucleoli. Higher magnification view of the previous slide. Most glands have occluded lumens. The nuclei are hyperchromatic.
Gleason 4 • - Incomplete gland formation • Several histological appearances: • - sometimes glands appear fused, sharing a common cell border • - sheets of cell nests or long cords of cells • - cribriform glands (large masses, ragged borders w/ infiltrating fingerlike projections
The glands are fused and there is no intervening stroma. Glandular fusion is a hallmark of Gleason grade 4. Higher magnification view of the previous slide. Most glands have occluded lumens. The nuclei are hyperchromatic.
Gleason 5 • - single infiltrating cells, no gland formation or lumen appearance • comedocarcinoma • cribriform glands w/ central areas of necrosis